
What ya Know About Obesity?
By: Kenleigh Benoit
What is Obesity?
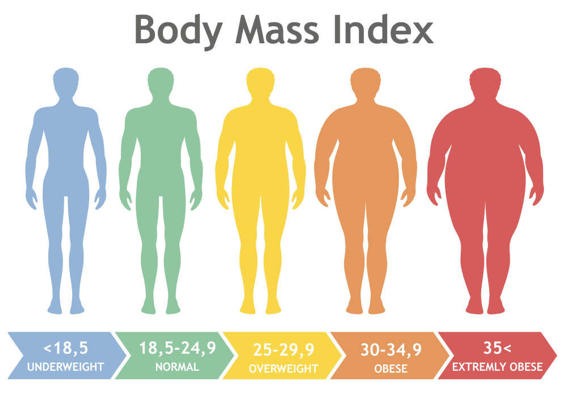
The term “obesity” is tossed around lightly as we do not realize just how serious the problem is. One is considered obese when their BMI (Body Mass Index) is 30 or above. The Body Mass Index is one’s weight in kilograms divided by the square of height in meters. This number indicates if a person has high body fatness. A person’s BMI is an accurate indicator of obesity because it takes into account one’s height and weight to determine if they are overweight.(3) Obesity is a serious health problem that causes an estimated 2.8 million deaths around the world each year.(7) In 2016, more than 650 million adults were considered obese and this number is only growing.(7) America, being a highly developed country, is a leading country in obesity rates as two out of every three adults are considered overweight or obese.(3) Many people are quick to place the blame on the person for obesity as they do not realize that obesity is also often inherited. Although there are many environmental factors that can affect one’s weight, there is a 64% to 84% attribute to genetics.(2)
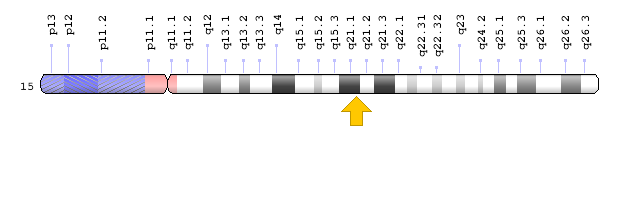
Your genes affect your susceptibility to many diseases and traits, including obesity. Although many of them have very small effects, there are over 50 genes associated with obesity.(2) For example, the APOA2 gene encodes the apoliprotein A-II protein. This protein affects our rates of lipid metabolism. The SNP, rs5082, occurs in the gene promoter and regulates the bodily response to an overload of saturated fat in men, leading to an increase in Body Mass Index and food intake.(2) Another SNP, rs1421085, is located on the FTO, a fat mass and obesity gene that promotes food intake, on chromosome 16. This makes sense that these variations change the structure of the proteins as this SNP disrupts certain processes, leading to a loss of mitochondrial thermogenesis. (2)
Why get Tested?
Obesity can cause heart disease, diabetes, and strokes, all of which are leading causes of death in the United States.(3) You should get tested for your genetic susceptibility to obesity because there are so many diseases that could result from it. With the knowledge of your susceptibility, you can eat healthier and exercise accordingly to prevent diseases caused by obesity. If one takes the test who is not already obese, they have the option to take medication to lower blood pressure and prevent blood clots, which are two health problems related to obesity. (1) The test that I would recommend that reveals your genetic risk of acquiring obesity is only $50 and uses the PCR and gel electrophoresis method as it is cost effective and gives accurate results of an individual from birth onward.(5) For more accurate results, one may consider whole genome sequencing to get the most common alleles, but this test is very costly, exceeding $1325. (Case Study #12) I think it would be much more cost efficient to get the $50 test because obesity is caused by both genetics and external factors that can be controlled. Unless you have a dire problem with obesity, I would recommend taking the cheaper test that will yield similar results.
In the article on the genetic effect on obesity, author Vicky Stein claims that “In middle-aged people, those who had the highest scores weighed an average of almost 30 pounds more than those with the lowest genetic risk. The high-scoring participants were 25 times as likely to develop severe obesity as low-scoring people, and their odds of diabetes, high blood pressure, heart disease, stroke and venous thromboembolism (a dangerous blood clot condition) increased as well.”(5) 30 pounds is a notable difference and knowing that you carry these risk alleles can help you create a custom health plan with your doctors to prevent obesity and disease.
What are the limitations of taking this test?
Since the risk alleles only account for about 3 kg/m2 of you Body Mass Index, one may decide to not partake in this genetic test as it is proved to not be useful. It is difficult to find the exact base risk as obesity is affected by outside factors along with genetics. Scientists have trouble finding the fine line between the two. The professors in the study, Is Genetic Testing of Value in Predicting and Treating Obesity?, claim that “The current set of identified common variants has poor specificity and poor sensitivity for predicting obesity in both cross-sectional and longitudinal studies.”(1) The idea that obesity is also caused by your genes is relatively new as most people thought it was solely based on what you eat and how much you exercise. Therefore, there are more than likely many variations in our DNA that scientists have not discovered a relation to obesity yet. The field is growing, so it may be influential to get the test in the future. Although genetic test for variants that causes obesity are not yet accurate, one could get a genetic test for hypothyroidism, a disease that disrupts one’s heart rate and metabolism that leads to unexplained weight gain.
What are the Ethical Concerns?
Although obesity is a leading cause of death, it is less than a concern than say cancer or heart disease because you can work to prevent obesity regardless of your genes, which only make the process more difficult. Financially, one may have to purchase medicine and, in severe cases, surgery. This could potentially be very costly. They may also choose to partake in personalized therapy to decrease their body weight. It is also slightly more costly to purchase healthier foods. Emotionally, I believe that a person would choose to strive to live a healthy lifestyle after learning of their susceptibility to obesity.(1) Likewise, It may be a somewhat frightful realization as obesity leads to so many detrimental diseases and cancers that could very likely lead to death.(6) If anything, a positive genetic test for obesity would make them adapt healthier habits to prevent these diseases.
There are many genetic privacy concerns that the person would have to consider. Many scientists use the results from genetic tests to discover which variants and alleles cause diseases, so they can prevent disease before it spreads. This is found through projects such as the Human Genome Project in which large amounts of people share their genetic information, but the patient could always opt to keep their results private. Other negative aspects of getting this genetic test would be one may learn that they are prone to obesity and not try to exercise to stay fit as they think it is inevitable that they will gain weight because of their genetics.
People respond to the results of genetic test differently. In a study called Parent Perspectives on Pediatric Genetic Research and Implications for Genotype-driven Research Recruitment. Some parents claimed they “wanted to help their affected child and felt that research was one way to feel like they were “doing something” in the context of uncertainty about the disease and treatment.”(6) Parents all inherently want to ensure the safety of their child and if genetic test will do so, then they are in support of it. Especially with a case like obesity, learning of your child’s susceptibility will make you more aware as a parent when feeding them or helping them stay active. This is something they can prevent by taking action when the child is very young. Other parents worry of the psychological impacts on themselves and their child. They argued that “Some people cannot handle knowing what may happen to them…they can get into some anxiety by thinking this will happen down the road to them, and that’s not helping.”(6) I agree with this sentiment for high risk diseases such as heart disease and cancer genes, but I think the positive results for obesity would not stress a child out. I think it will ultimately make them pay more attention to how they are living their life.
Could you be susceptible to obesity?
- Do you find yourself gaining weight at unreasonable rates?
- Are your parents or other family members considered to be obese?
- Do you see yourself as a “normal” eater and are still gaining weight?
- Do you exercise adequately and still have serious weight problems?

If you said yes to these questions, then you may have genetic mutations that make you predisposed to obesity. Does anyone in your family struggle with obesity? If so, you may be more susceptible to obesity and taking a genetic test may be needed to maintain your health. If you possess variants that make you susceptible to obesity, you should consider a genetic test for your child at birth as they have a 50% chance of acquiring that same trait. It is somewhat rare to acquire obesity through inheritance as it is often caused by environmental and lifestyle choices. It is not likely that you will get the trait from extended family members such as your aunt.
Obesity can lead to other diseases such as diabetes, depression, cancer, and heart disease. It is best to tackle the problem immediately. If the test came back negative, they should still maintain their health even though they are not genetically susceptible to the disease. I believe it is very wise to consult your results with your doctor if you test positive as they have knowledge of how to successfully fight obesity. I would tell my doctor that I tested positive for obesity and ask what steps I needed to take to lose weight and be healthier. I would also ask about the risk of getting other diseases because of my susceptibility to obesity.
There are many environmental factors that affect obesity. If I tested positive for obesity, I would change my daily intake, exercise routine, and diet. The combination of these changes would lead to a healthier lifestyle altogether. I recommend getting screenings for diabetes, high blood pressure, high cholesterol, and heart disease if you tested positive for obesity as this puts you at risk for many illnesses. If you believe you may be susceptible to obesity, do not hesitate in taking a genetic test. Obesity is extremely harmful as it leads to so many deathly illnesses, disorders, and diseases. We must care for our bodies by living a healthy lifestyle with exercise and a fulfilling, clean diet no matter what our genes decide for us.
Resources
(1)Bowden, D. W., Maggie C. Y., (2013). Is Genetic Testing of Value in Predicting and Treating Obesity? U.S. National Library of Medicine National Institutes of Health, 74(6): 530–533.
(2)Obesity. (2017, May 10). Retrieved November 13,2019, from https://www.snpedia.com/index.php/Obesity.
(3)Ogden, C. (2017, August 1). Overweight and Obesity Statistics. Retrieved November 13,2019, from https://www.niddk.nih.gov/health-information/health-statistics/overweight-obesity.
(4)Overweight & Obesity Statistics. (2013, May 17). Retreived Novemebr 13, 2019, from https://www.niddk.nih.gov/health-infomration/health-statistics/overweight-obesity.
(5) Stein, V. (2019, April 18). This genetic test can predict your odds for obesity from the day you’re born. Retrieved December 2, 2019, from https://www.pbs.org/newshour/science/this-genetic-test-can-predict-your-odds-for-obesity-from-the-day-youre-born.
(6)Tabor, H. K., Brazg, T., Crouch, J., Namey, E. E., Fullerton, S. M., Beskow, L. M., & Wilfond, B. S. (2011). Parent Perspectives on Pediatric Genetic Research and Implications for Genotype-Driven Research Recruitment. Journal of Empirical Research on Human Research Ethics, 6(4), 41–52. doi: 10.1525/jer.2011.6.4.41.
(7)10 facts on obesity. (2017, October). World Health Organization. Retrieved November 13th, 2019, from https://www.who.int/features/factfiles/obesity/en/.













{kind=link}
{kind=link}
{kind=link}