Huntington’s Disease is an inherited neurological illness. About 30,00 people in the United States have the disease (1). It is caused by a mutation on the HD gene, that codes for huntingtin protein production which has much more repeats than normal of a certain three-basese sequence (1). This gene is located on the fourth chromosome. It causes the degeneration of nerve cells in the brain that leads to symptoms such as changes in behavior and judgement, uncontrollable movement and physical changes such as impaired ability to swallow or speak (3).
For a predictive genetic test, the price is $200-$300. There is recommended genetic counseling that can cost up to $1,500-$2,000 (4). The most effective test is a direct-to-consumer genetic test that counts the extra repeats of the three base sequence in the Huntington gene on the fourth chromosome through a blood sample (3). The test could use a method such as the Southern Blot method. There is a very strong, almost definitive connection between the mutation in the fourth chromosome that would be tested for, and the disease.
With the direct genetic test, there is a small amount of people who have a borderline amount of repeats. Their family may be called in for genetic testing as well to get a better picture. Huntington’s can be ruled out if there are 26 or fewer repeats (3). The test can’t predict when the symptoms will start or the course of the disease (2).
There are many potential implications if the genetic testing is positive for Huntington’s Disease. There may be personal stress and possible distress to those close to the person with Huntington’s Disease. Also, Huntington’s does not have a cure. Therefore, there is no medical advantage to knowing the test results. You can only treat the symptoms as they appear. You can, however, plan for the future and factor that into any family planning decisions. The Genetic Information Non Discrimination Act (GINA) is a law that was made to stop discrimination from based on genetic information with health insurance. Although it applies to health insurance, it does not apply to life insurance so a positive test may raise prices for life insurance dramatically or may not allow for getting a policy at all. (2)
Since Huntington’s is an autosomal dominant disease, the chances of getting it if even one parent has HD will be fairly high. If both the parents have recessive alleles, the offspring will not get the disease. However, if you have two heterozygous, there’s a 75% chance of getting the disease. If one parent is heterozygous and one homozygous recessive, there’s a 50% chance. If one parent is heterozygous and one homozygous dominant, there’s a 100% chance of getting the disease. If the test is positive, the person should make a plan for the future and be prepared to address the symptoms as they come. I would recommend telling the doctor that the test was positive and ask if they have any suggestions on how to proceed.
Overall, Huntington’s Disease is an incurable disease with limited reasons to test for it. Since it is a dominant disease, there is a small chance of one developing it if it does not run through the family. Although not too complicated to test for, the consequences of a positive result outweigh the benefits in most cases.
Works Cited:
About Huntington’s Disease. (2011, November 17). Retrieved from
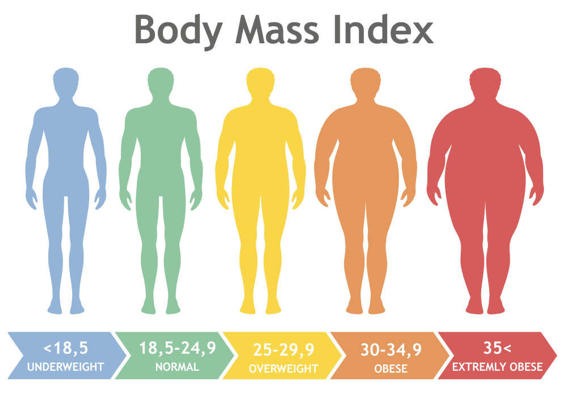
The term “obesity” is tossed around lightly as we do not realize just how serious the problem is. One is considered obese when their BMI (Body Mass Index) is 30 or above. The Body Mass Index is one’s weight in kilograms divided by the square of height in meters. This number indicates if a person has high body fatness. A person’s BMI is an accurate indicator of obesity because it takes into account one’s height and weight to determine if they are overweight.(3) Obesity is a serious health problem that causes an estimated 2.8 million deaths around the world each year.(7) In 2016, more than 650 million adults were considered obese and this number is only growing.(7) America, being a highly developed country, is a leading country in obesity rates as two out of every three adults are considered overweight or obese.(3) Many people are quick to place the blame on the person for obesity as they do not realize that obesity is also often inherited. Although there are many environmental factors that can affect one’s weight, there is a 64% to 84% attribute to genetics.(2)
Your genes affect your susceptibility to many diseases and traits, including obesity. Although many of them have very small effects, there are over 50 genes associated with obesity.(2) For example, the APOA2 gene encodes the apoliprotein A-II protein. This protein affects our rates of lipid metabolism. The SNP, rs5082, occurs in the gene promoter and regulates the bodily response to an overload of saturated fat in men, leading to an increase in Body Mass Index and food intake.(2) Another SNP, rs1421085, is located on the FTO, a fat mass and obesity gene that promotes food intake, on chromosome 16. This makes sense that these variations change the structure of the proteins as this SNP disrupts certain processes, leading to a loss of mitochondrial thermogenesis. (2)
Why
get Tested?
Obesity can cause heart disease, diabetes, and strokes, all of which are leading causes of death in the United States.(3) You should get tested for your genetic susceptibility to obesity because there are so many diseases that could result from it. With the knowledge of your susceptibility, you can eat healthier and exercise accordingly to prevent diseases caused by obesity. If one takes the test who is not already obese, they have the option to take medication to lower blood pressure and prevent blood clots, which are two health problems related to obesity. (1) The test that I would recommend that reveals your genetic risk of acquiring obesity is only $50 and uses the PCR and gel electrophoresis method as it is cost effective and gives accurate results of an individual from birth onward.(5) For more accurate results, one may consider whole genome sequencing to get the most common alleles, but this test is very costly, exceeding $1325. (Case Study #12) I think it would be much more cost efficient to get the $50 test because obesity is caused by both genetics and external factors that can be controlled. Unless you have a dire problem with obesity, I would recommend taking the cheaper test that will yield similar results.
In the article on the genetic effect on obesity, author Vicky Stein claims that “In middle-aged people, those who had the highest scores weighed an average of almost 30 pounds more than those with the lowest genetic risk. The high-scoring participants were 25 times as likely to develop severe obesity as low-scoring people, and their odds of diabetes, high blood pressure, heart disease, stroke and venous thromboembolism (a dangerous blood clot condition) increased as well.”(5) 30 pounds is a notable difference and knowing that you carry these risk alleles can help you create a custom health plan with your doctors to prevent obesity and disease.
What are the limitations of taking this test?
Since the risk alleles only account for about 3 kg/m2 of you Body Mass Index, one may decide to not partake in this genetic test as it is proved to not be useful. It is difficult to find the exact base risk as obesity is affected by outside factors along with genetics. Scientists have trouble finding the fine line between the two. The professors in the study, Is Genetic Testing of Value in Predicting and Treating Obesity?, claim that “The current set of identified common variants has poor specificity and poor sensitivity for predicting obesity in both cross-sectional and longitudinal studies.”(1) The idea that obesity is also caused by your genes is relatively new as most people thought it was solely based on what you eat and how much you exercise. Therefore, there are more than likely many variations in our DNA that scientists have not discovered a relation to obesity yet. The field is growing, so it may be influential to get the test in the future. Although genetic test for variants that causes obesity are not yet accurate, one could get a genetic test for hypothyroidism, a disease that disrupts one’s heart rate and metabolism that leads to unexplained weight gain.
What are the Ethical Concerns?
Although obesity is a leading cause
of death, it is less than a concern than say cancer or heart disease because
you can work to prevent obesity regardless of your genes, which only make the
process more difficult. Financially, one may have to purchase medicine and, in
severe cases, surgery. This could potentially be very costly. They may also
choose to partake in personalized therapy to decrease their body weight. It is
also slightly more costly to purchase healthier foods. Emotionally, I believe
that a person would choose to strive to live a healthy lifestyle after learning
of their susceptibility to obesity.(1) Likewise, It may be a
somewhat frightful realization as obesity leads to so many detrimental diseases
and cancers that could very likely lead to death.(6) If anything, a
positive genetic test for obesity would make them adapt healthier habits to
prevent these diseases.
There are many genetic privacy concerns that the person would have to consider. Many scientists use the results from genetic tests to discover which variants and alleles cause diseases, so they can prevent disease before it spreads. This is found through projects such as the Human Genome Project in which large amounts of people share their genetic information, but the patient could always opt to keep their results private. Other negative aspects of getting this genetic test would be one may learn that they are prone to obesity and not try to exercise to stay fit as they think it is inevitable that they will gain weight because of their genetics.
People respond to the results of genetic test differently. In a study called Parent Perspectives on Pediatric Genetic Research and Implications for Genotype-driven Research Recruitment. Some parents claimed they “wanted to help their affected child and felt that research was one way to feel like they were “doing something” in the context of uncertainty about the disease and treatment.”(6) Parents all inherently want to ensure the safety of their child and if genetic test will do so, then they are in support of it. Especially with a case like obesity, learning of your child’s susceptibility will make you more aware as a parent when feeding them or helping them stay active. This is something they can prevent by taking action when the child is very young. Other parents worry of the psychological impacts on themselves and their child. They argued that “Some people cannot handle knowing what may happen to them…they can get into some anxiety by thinking this will happen down the road to them, and that’s not helping.”(6) I agree with this sentiment for high risk diseases such as heart disease and cancer genes, but I think the positive results for obesity would not stress a child out. I think it will ultimately make them pay more attention to how they are living their life.
Could
you be susceptible to obesity?
Do you find yourself gaining weight at unreasonable rates?
Are your parents or other family members considered to be
obese?
Do you see yourself as a “normal” eater and are still gaining
weight?
Do you exercise adequately and still have serious weight
problems?
If you said yes to these questions, then you may have genetic mutations that make you predisposed to obesity. Does anyone in your family struggle with obesity? If so, you may be more susceptible to obesity and taking a genetic test may be needed to maintain your health. If you possess variants that make you susceptible to obesity, you should consider a genetic test for your child at birth as they have a 50% chance of acquiring that same trait. It is somewhat rare to acquire obesity through inheritance as it is often caused by environmental and lifestyle choices. It is not likely that you will get the trait from extended family members such as your aunt.
Obesity can lead to other diseases such as diabetes, depression, cancer, and heart disease. It is best to tackle the problem immediately. If the test came back negative, they should still maintain their health even though they are not genetically susceptible to the disease. I believe it is very wise to consult your results with your doctor if you test positive as they have knowledge of how to successfully fight obesity. I would tell my doctor that I tested positive for obesity and ask what steps I needed to take to lose weight and be healthier. I would also ask about the risk of getting other diseases because of my susceptibility to obesity.
There are many environmental factors that affect obesity. If I tested positive for obesity, I would change my daily intake, exercise routine, and diet. The combination of these changes would lead to a healthier lifestyle altogether. I recommend getting screenings for diabetes, high blood pressure, high cholesterol, and heart disease if you tested positive for obesity as this puts you at risk for many illnesses. If you believe you may be susceptible to obesity, do not hesitate in taking a genetic test. Obesity is extremely harmful as it leads to so many deathly illnesses, disorders, and diseases. We must care for our bodies by living a healthy lifestyle with exercise and a fulfilling, clean diet no matter what our genes decide for us.
Resources
(1)Bowden, D. W., Maggie C. Y., (2013). Is Genetic Testing of Value
in Predicting and Treating Obesity? U.S. National Library of Medicine
National Institutes of Health, 74(6): 530–533.
(3)Ogden,
C. (2017, August 1). Overweight and Obesity Statistics. Retrieved November
13,2019, from https://www.niddk.nih.gov/health-information/health-statistics/overweight-obesity.
(5) Stein,
V. (2019, April 18). This genetic test can predict your odds for obesity from
the day you’re born. Retrieved December 2, 2019, from
https://www.pbs.org/newshour/science/this-genetic-test-can-predict-your-odds-for-obesity-from-the-day-youre-born.
(6)Tabor, H. K., Brazg, T.,
Crouch, J., Namey, E. E., Fullerton, S. M., Beskow, L. M., & Wilfond, B. S.
(2011). Parent Perspectives on Pediatric Genetic Research and Implications for
Genotype-Driven Research Recruitment. Journal of Empirical Research on
Human Research Ethics, 6(4), 41–52. doi:
10.1525/jer.2011.6.4.41.
(7)10
facts on obesity. (2017, October). World Health Organization. Retrieved
November 13th, 2019, from https://www.who.int/features/factfiles/obesity/en/.
Alcohol
dependence, also known as alcoholism, is a form of alcohol addiction where the
individual has a physical dependence on the consumption of alcohol. This
physical dependence causes individuals to consume more alcohol than individuals
who do not have a dependence on alcohol, which further increases the health
risks of alcohol. Some of these risks include high blood pressure, stroke, and
liver cancer. Furthermore, according to the National Institute of Health (NIH),
individuals with alcoholism are more vulnerable to diseases such as tuberculosis
and pneumonia. This is because alcohol can weaken the immune system. Every
year, over 3.3 million individuals die worldwide due to alcoholism. This is the
third highest cause of preventable deaths, behind smoking and overeating. In
addition, according to data from 2009, approximately 3.5% of cancer deaths in the
United States was caused by alcohol.
According to
SNPedia, there are six known SNPs that affect the likelihood that an individual
will suffer from alcoholism. One example of these SNPs is rs1799971, where the
rs1799971 (G) variant increases one’s cravings for alcohol compared to the
normal allele, rs1799971 (A) for both carriers and individuals with two G
alleles. However, for individuals with the G variant, they respond to
naltrexone treatment better than those with the A variant.
Testing
for alcoholism
Some individuals
may experience more severe symptoms as a result of alcoholism, such as seizures
and increased risk for ADHD. For those who are concerned about such symptoms,
they should take a genetic test to see if they have an increased likelihood of
suffering from such symptoms. Because there are two SNPs, rs27048 and rs27072,
that are associated with such severe symptoms, an SNP test, which does not need
to be a whole sequencing test, will produce the best results at the lowest
costs, such as a $199 23andme test. However, if anyone is interested in whether
he or she has an increased risk of alcoholism in general, a $599 Veritas test
works best. However, a test specifically for rs1076560 (A), which is the most
common allele that increases the risk of alcoholism, also works well. Carriers
of this allele are 30% more at risk of becoming an alcoholic compared to
individuals who have two rs1076560 (C) alleles. The tests will satisfy the
needs of those who are interested in such information, as there is enough
evidence to conclude that an increased risk of alcoholism has correlations with
genetics. Despite the evidence, however, having an allele that increases the risk
for alcoholism does not guarantee that one will become an alcoholic, nor does
it guarantee that one will develop the more severe symptoms, such as ADHD, as
the risks of having certain alleles are probability-based, rather than a
guarantee. For instance, while data shows that a carrier of the rs1076560 (A)
allele is 30% more likely to become an alcoholic, this does not mean that he or
she will be an alcoholic automatically because he or she drank one sip of beer.
Furthermore, there are some contradictory studies against the idea that
rs1799971 has anything to do with alcoholism.
Ethical
Concerns
According to
the National Institutes of Health, the majority of participants in a study
regarding the effects of genetics on alcoholism were more concerned about
discrimination from their physician (approximately 40%), rather than their
family and friends (approx. 29%). Therefore, if participants are considering
such a test, then they should evaluate whether they would feel comfortable
around their physician after taking such a test.
Testing
Positive
If someone
tests positive in regards to any of the alleles that increase the risk of
alcoholism, then his or her has a likelihood of inheriting this risk, as these
alleles are hereditary. In order to better manage this risk, he or she can contact
the Addiction Center for advice. Rehabilitation treatment from the Addiction
Center is not necessary, unless he or she already has an alcohol addiction. However,
if anyone tests positive, then he or she should not be forbidden to drink as
long as he or she follows the rules that pertain to drinking, such as not
drinking until 21 and avoiding the behavior of drunk driving. Heavier
self-restraint, however, is advised, and abstinence is recommended. If an
individual has a rs1799971 (G) allele and is suffering from alcoholism, then he
or she should consult a doctor because individuals with this allele, despite
having an increased risk of alcoholism, respond better to naltrexone treatment
than normal individuals do.
Sources
Scott, D. M. et al.
(2014, August). Genetic testing for the susceptibility to alcohol
dependence: interest and concerns in an
African American population. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4120651/
Men these days are
judged ever increasingly more by their appearance; we need to be fit, handsome,
well-dressed, and well-groomed. If we fail in any of these categories, we are
instantly judged to be inferior. These are all important things to take care of,
but perhaps no other physical characteristic exceeds the challenges posed by
one’s own head of hair. Yes, it is our luscious locks that drive men to
insanity about their appearance. But the insanity doesn’t set in until the hair
follicles begin to fall out.
We are talking about male pattern baldness.
From thinning hair to a receding hair line, the condition can be devastating to a man’s self esteem and may even be linked to certain health conditions other than balding! With so much on the line, is there any way of predicting if you will develop male pattern baldness? And if so, is it even worth it? We will explore these questions and more in this blog.
WHAT IS MALE PATTERN BALDNESS?
Male pattern baldness is an inherited condition that
results in the loss of significant amounts of head hair follicles. Symptoms
include thinning hair, patchy bald spots, and a receding hair line1.
According to a 2017 study by Hagenaars and colleagues, male pattern baldness affects as much as 80% of men by the time they reach 80 years old. The dramatic and unstoppable change associated with this condition is often depressing and difficult to watch for many men, not to mention its damage to their perceived social attractiveness. The same 2017 study also found 112 autosomal genes as well as 13 genes located on the X chromosome that all are associated with male pattern baldness. Several of the autosomal genes are related to hair follicle growth while the most common X chromosome gene codes for androgen reception2. The genes linked with male pattern baldness naturally make sense. Because the condition concerns the loss of hair follicles, genes that cause male pattern baldness to develop must have some role in hair development. Furthermore, the fact that the androgen receptor gene is correlated with baldness raises the question that some hormonal process must be involved, which explains the sudden change that occurs.
Above is a man with moderate male pattern baldness. Notice the thinning hair and the bald spot1
WHY GET TESTED?
Since male pattern baldness is such a prevalent and unavoidable condition, why would one want to get genetically tested for it? If it is going to happen, then it will happen, right? For many, the emotional trauma of suddenly losing his hair is awful. But early-onset male baldness has been linked with several particularly nasty diseases, including prostate cancer and Parkinson’s disease3. As a result, getting tested early can provide relative peace-of-mind for those labeled as “low risk” and provide those labeled as “high risk” with plenty of time to prepare and start preventative measures, like prostate exams or even looking into alternatives to balding, like hair transplants.
Since there is such a massive number of genes and alleles
that appear to cause male pattern baldness, it would perhaps be best to get a
genome-wide sequencing test in order to detect as many of the potential
variations as possible. This type of test typically runs around $1,5004.
For the most common alleles, it would be cheaper
simply to test those specific genes. These tests cost approximately $220 for
the entire gene, but for more than just one, it becomes more cost-effective to
do the whole genome sequencing.
The previously mentioned 2017 study found a much
higher frequency of certain variations of an X chromosome gene in men with
early-onset balding than with late-onset. Therefore, it is possible to
genetically test for the risk of developing early-onset male pattern baldness.
In a 2012 study by Li and colleagues,Parkinson’s and early-onset male pattern baldness were found to
be linked by one specific allele on chromosome 175.Getting tested
may be worth it for both the peace-of-mind of keeping one’s hair and not
developing Parkinson’s.
THINK BEFORE YOU
SPIT
A genetic test, unfortunately, is not exactly a
crystal ball. Simply having the genetic variations associated with male pattern
baldness is not enough to declare that a subject will become bald. Only 51.9%
of the variation in the human population with respect to baldness can be
explained by the genetic variants found the Hagenaars et al study2.
Some factors that may affect baldness outside of genes include weight, stress,
chemotherapy treatment, and even simply getting older1.
Furthermore, there may be even more variations that
have not been detected yet. Research on the genetics of male pattern baldness
is still relatively lacking3, so the potential for more (or even
fewer) variants that cause balding is possible.
ETHICAL
CONSIDERATIONS
Testing as a “high risk” candidate for balding will
be terribly worrying for any man placed in such a situation. Given the possible
correlations with various diseases, it would be hard not to stress over the
test’s findings. Ignoring the potential for disease, even losing one’s hair, a
symbol of one’s male identity, fills many with dread about future social and
physical decline.
Luckily, there appear to be no major or common
concerns for genetic privacy. Few companies would discriminate against an
employee given his genetic propensity for balding, save those of the
entertainment and modeling industry. As a result, few men should worry if
getting tested for male pattern baldness might damage his prospects for future
employment.
There are other downsides, though, to consider. Given the cost and potential for inaccuracy
in predicting risk of developing male pattern baldness, it may not be worth the
$1,500 to sequence one’s entire genome. However, there is an added bonus. Once
a genome has been sequenced, it will be available in its entirety for further
analysis of other potential diseases, like risks for certain cancers. Even if
the balding prediction does not hold true, having the option to also check for
those awful diseases might just be worth it.
ASKING THE RIGHT
QUESTIONS BEFORE THE TEST
In order to determine if genetic testing is right
for you, here are some important questions to consider.
Do you have a family history of balding, on either side?
This is important to ask because if not,
then there is very little chance that the cause of any balding you might have
in the future will be due to genetics.
What will you do
if you test as a high-risk individual?
If you cannot answer what you would do
after being labeled as high-risk for balding, then perhaps the genetic test is
not right for you. It is too expensive to simply do it for the peace-of-mind;
it is best to go into the test with a plan for either treatment (if desired) or
coping with balding.
What will you do
if you test as a low-risk individual?
Being labeled as a low-risk individual
does not necessarily mean you are in the clear. You may still develop male
pattern baldness in the future. On another note, you need to still continue to
remain healthy as general health can also affect hair loss.
Consider
discussing getting the test and the results of the test with a doctor or
geneticist.
Not so much a question as much as
advice. If you would like to explore being tested, it would be wise to discuss
your risks of balding before spending all that money on the test. Furthermore,
if you have been tested and would like to consider potential treatment options
and/or other genetic risks, doctors and geneticists are excellent resources to
find out more about such topics.
What are you willing
to change after being identified as high-risk?
To reduce your overall chances of
developing baldness even after being labeled as high-risk, it is important to
try to be healthy and fit. To even further reduce risk, it may be best to
consider changing your hairstyle, which can damage hair follicles, or trying to
reduce stress, which can induce hair loss.
Regardless of whether you decide it is best to get tested for male pattern baldness, it is important to maintain a healthy sense of what matters. If you are legitimately concerned about your appearance and you actively want to prevent losing your hair, then getting genetically tested is not a bad idea. But if you honestly don’t mind the prospect of balding, then that’s ok too! It is all a personal choice; no two people will have the same reasons for either decision. And regardless of that decision, above all, you need to learn to love who you are, whether that’s with a full head of hair or none at all.
5Li
R, Brockschmidt FF, Kiefer AK, et al.Six novel susceptibility Loci
for early-onset androgenetic alopecia and their unexpected association with
common diseases. PLoS Genetics. 2012. https://www.ncbi.nlm.nih.gov/pubmed/22693459/.
Accessed December 2, 2017.
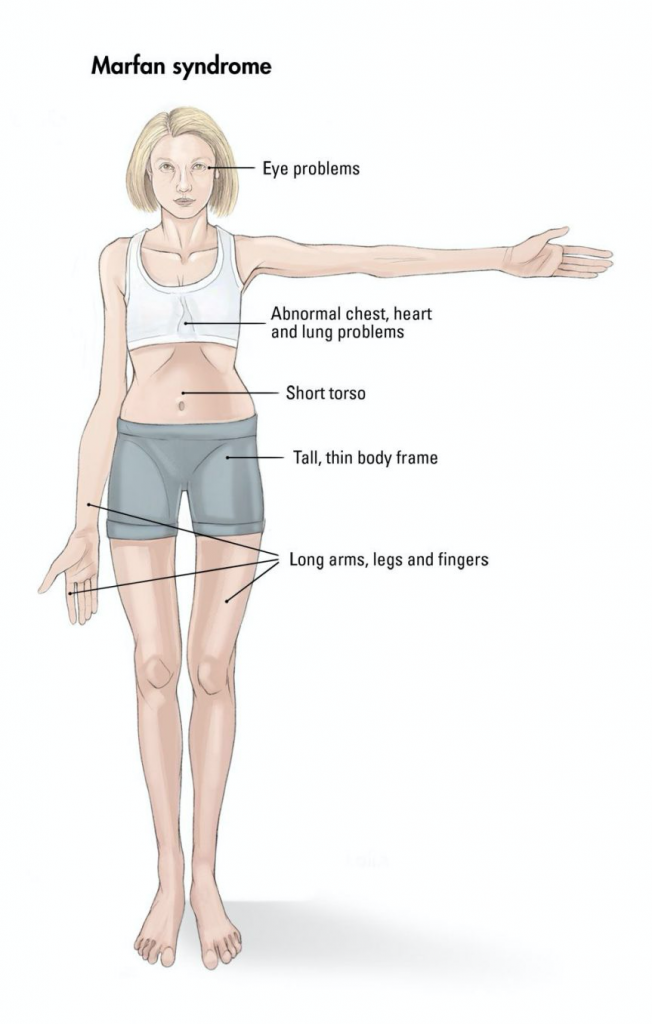
The trait I am testing for is Marfan Sydrome, an inherited genetic disease caused by a mutation in the FBN1 gene. While not very common, only occurring in around one in five thousand people (NIH), Marfan’s main symptoms are elongated limbs, worsened vision and heart issues. Only one gene is known to be the cause, and it can result from a change in any of the many alleles within the gene.
Marfan affects the production of fibrillin, a compound key to the extracelluar matrix and skeletal and muscular development1. The condition causes the afflicted to be taller than average, along with having thin arms and legs and possible heart issues. The above average height of those with Marfan can be very beneficial for athletes, especially basketball and volleyball players. Famous atheletes with Marfan include Olympic medalist Flo Hyman and basketball player Isaiah Austin. As the mutation affects the above developments, it makes sense that those carrying it have thinner, weaker muscles due to a less strong extracelluar matrix which provides support around cells through a compound called fibrillin. Marfan leads to decreased fibrillin production, and thus less strength and elacticity in tendons and muscles. This leads to those with Marfan tending to have longer, slimmer limbs and aorta issues in the heart.
Testing for Marfan would more than likely be done to test for the likelihood of the disease in offspring. The condition is not always obvious, depending on the severity of symptoms. A SNP-ChiP is best recommended, as this test can encompass the entire gene and detect any and all SNPs which have mutated, leading to the affliction2. There is no specific allele or SNP known as the cause, many different ones from FBN1 have been seen to cause Marfan3. This test can run anywhere from $200-$2000, depending on insurance and the laboratory running the test. There is a very strong connection between these mutations and the disease, as over a thousand alleles have been tied to it4 and if you have the mutation you will demonstrably have the disease. Getting a test done is most effective to determine risk in newborns to see if they will later develop symptoms. The risk of inheritance is fifty percent if one parent has the condition as it is autosomal dominant and those who carry the mutation are at a one hundred percent risk of developing symptoms.
Testing is not necessarily needed for this condition, but may be beneficial. Those who have any of the mutations will in many cases show symptoms and thus not need testing. Parents, however, can use testing to segregate eggs which do not carry a mutation and selectively breed children through invitro fertilization. The ethics around this are murky and can cause controversy. Adults with the condition commonly know they carry it and do not need to give up genetic information to a company just to discover they have a mutated allele they already knew about. From a scientific point of view, testing is not commonly needed. Those with symptoms should strongly consider getting tested. The main possible benefit would be that a positive would indicate possible heart issues, and further testing could be done. Getting a test done could also be beneficial for those without symptoms, as they may not visibly show it but could have Marfan and potentially develop complications. There are few ethical concerns around this kind of testing, with the only main exception being around in-vitro fertilization and selective breeding.
Family history plays a large part into having Marfan. If one parent has it, the child will have a fifty percent chance of having it as it is an autosomal dominant condition. Marfan is only inherited directly from an afflicted parent. One has a roughly one in twenty thousand chance of randomly developing it. There are no needed environmental adjustments needed if the test is positive however, as the disease is not affected by the environment. A positive or negative result from the test is only significant for a child who has not yet developed symptoms or for an adult with onlt one symptom. As Marfan is untreatable, in this case the parents could try to mitigate symptoms, but they cannot be fully treated. Adults who show as positive could also get screened for heart issues which are commonly tied to Marfan.
References
1. NIH. (2019, November 12). Marfan Syndrome. Retrieved from https://www.nhlbi.nih.gov/health-topics/marfan-syndrome#.
2. Singh et al. (2015). Single-copy gene based 50 K SNP chip for genetic studies and molecular breeding in rice. Scientific Reports, 5(1). doi: 10.1038/srep11600
3. Mayo Clinic. (n.d.). Test ID: FBN1B FBN1 Full Gene Sequence, Varies. Retrieved from https://www.mayocliniclabs.com/test-catalog/Clinical and Interpretive/64514.
What do we think of when we think about rare diseases? Well first of all, they’re rare: no one around me has it, my parents don’t have it, chances are, I won’t get it, nor will my children get it. Which means I don’t have to worry about getting it myself then, right?
Well let’s consider this disease: Fatal Familial Insomnia (FFI). FFI is the rarest known prion disease today – only 25 families are known to have it (2). The symptoms of the disease are initially mild – usually just an inability to sleep. As time progresses, however, there will be significant mental deterioration: dementia, problems with cognition and thought, and “dysfunction of the autonomic nervous system” (5). This impacts the human body’s ability to maintain body temperature, heart rate, and blood pressure (5). This mental deterioration continues for about a year or so until “the disease ultimately progresses to coma and death” (5).
But even as horrifying as that seems, as long as we aren’t one of the 25 families, we don’t have to worry about the disease, right? Unfortunately, it doesn’t seem completely so – in 2004, doctors studied the case of a man with the disease who was of Chinese descent – the first case of FFI ever in the Chinese population (9). This means that the disease can still occur anywhere. But ultimately, so little is known about it that scientists are struggling to find a complete explanation – and indeed, a cure – for this rare disease. Even if you don’t think you have it, getting tested for the FFI gene can provide scientists with the information they need to find the origin of the disease, and how to treat and cure it.
So what is the disease?
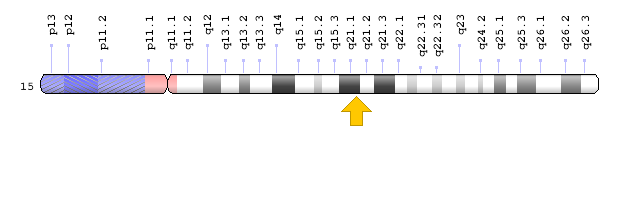
FFI is known as a Prion disease. These kinds of diseases occur when the PRNP gene, a gene which controls the creation of prion protein, has a mutation (5). This mutation causes the gene to create misfolded prion protein – these prion proteins are toxic and will build up in the brain, destroying important nerve cells, leading to the symptoms of the disease (5).
So far, the mutations is the genes are from SNP’s, where one small segment of the DNA is switched. D178N is a SNP for residue 178 in the PRNP gene (8). Another SNP is the M129V SNP, also in the PRNP gene (6). The last SNP is the E200K mutation, which is a common prion disease mutation (7). It’s very possible for the change in the PRNP gene, which directly creates the prion protein, to affect the prion’s shape – other prion related diseases stem from these mutations too (6).
Once someone has the disease, the disease itself is autosomal-dominant (5). That means if a parent has it, there is at least a 50% chance of the children having it too. In the case of the Canadian family mentioned before, the disease traced through the family, like the patient’s aunt (9). Since many of the patients who had the disease didn’t start showing symptoms until later in life, such as the aunt in her late 40’s (9), it is highly possible for someone who has the disease to pass it to their children.
Image from the CJD Foundation (1).
So how can we test for it?
The best way to test for this disease would be to use traditional DNA sequencing. There is only one single gene to look at, and only at three points. All of them are SNPs, so it would be easy to know what to look for. For the three locations, the cost would be low, since there are so few of them. These mutations have a strong correlation with people who have the disease, such as D178N with a magnitude of 6.5 (8).
Unfortunately, getting the test may not be enough to prove if you have the disease or not. Because of it’s rarity, many of the mutations that can occur that will cause this disease, may not be known yet (5). It is still entirely possible to get this disease through some other mutation – take Sporadic Fatal Insomnia: this disease is the exact same as FFI, except it’s cases are completely random (4). So, even though the known SNP’s provide definitive proof of having the disease or not, the probability of having the disease is still not 0. In the end, it may be in the best interest of people, who have a family history of diseases with anything resembling the symptoms of FFI, to get tested for the disease. Even if they don’t think they have the disease, they may be some of the people with the closest connections to this disease.
What happens when I get tested?
With the rarity of the disease, most likely nothing. People who test negative for this disease will almost certainly never get it. But when they do test positive for it, it would be a horrible moment. Currently, there is no treatment for FFI; there have been so few cases, that researchers could not create a definitive treatment for it (5). Even if someone knows they have FFI, there is no definitive way to get rid of it. Once someone gets the disease, they may no longer want to keep it to themselves – the best hope to get it cured or treated would be to contact researchers for help.
If you do test positive, contact your doctor to let them know. They should know about your current condition, and if any medications you may have taken (5). If you have medication that makes any of the symptoms worse, you should stop taking them and ask your doctor if there are any alternatives (5). It is also possible to get scans done of your brain for activity, which can be especially helpful in determining where and what may be causing the symptoms (5). If you are interested in getting tested for this, ask yourself these questions: Do I have problems falling asleep? Am I experiencing forgetfulness? Do I have problems paying attention? Am I loosing weight faster than I expected? Does anyone in my family have these symptoms (5)?
Because of the lack of information about the disease, not many people know about it. However, if more people were to go and test for it, they may be able to help change that. Sonia and Eric have worked together to find a solution to the FFI disease after events in their life prompted them to do so (3). Testing for the gene doesn’t cost much, but its value is incredible for researchers. So even if it is highly unlikely for you to get this disease, just a little bit of time and money spent to get tested for this disease will help researchers save the lives of others.
Works Cited
1. Creutzfeldt-Jakob Disease Foundation, Inc. (n.d.). About CJD and Prion Disease. Retrieved from: https://cjdfoundation.org/about-cjd
4. Medori, R., at el. (1992, February 13). Fatal Familial Insomnia, a Prion Disease with a Mutation at Codon 178 of the Prion Protein Gene. Retrieved from: https://www.nejm.org/doi/full/10.1056/NEJM199202133260704
5. National Organization for Rare Disorders. (2018). Fatal Familial Insomnia. Retrieved from: https://rarediseases.org/rare-diseases/fatal-familial-insomnia/
6. SNPedia. (2018, January 6). rs1799990. Retrieved from: https://www.snpedia.com/index.php/Rs1799990
7. SNPedia. (2018, January 6). rs28933385. Retrieved from: https://www.snpedia.com/index.php/Rs28933385
8. SNPedia. (2019, January 18). rs74315403. Retrieved from: https://www.snpedia.com/index.php/Rs74315403
9. Spacey, S.D., Pastore, M., McGillivray, B., Fleming, J., Gambetti, P., & Howard, F. (2004, January). Fatal Familial Insomnia: The First Account in a Family of Chinese Descent. Retrieved from: https://jamanetwork.com/journals/jamaneurology/fullarticle/785214
What genes help to determine athletic performance?
The ACE and ACTN3 genes help determine what type of fibers an individual’s muscles are made up of, and whether they have more fast-twitch muscle fibers or slow-twitch muscle fibers. (2)
Fast-twitch muscle fibers can generate more power and contract more quickly and forcefully. Slow-twitch muscle fibers use oxygen more efficiently and tire more slowly. As a result, athletes who compete in strength/speed events (short-distance running) usually have more fast-twitch muscle fibers, while athletes who compete in endurance events (distance running) usually have more slow-twitch muscle fibers.
Usain Bolt competes in an event that tends to favor athletes with more fast-twitch fibers
Eliud Kipchoge competes in an event that tends to favor athletes with more slow-twitch fibers
ACE
ACE instructs cells to create angiotensin-converting enzyme, a protein that converts the angiotensin hormone from angiotensin I to angiotensin II. (2)
If an individual has a variant of ACE known as ACE I/D Polymorphism, then that individual may have a higher level of angiotensin-converting enzyme. Individuals can have one of three patterns: the II pattern, the ID pattern, and the DD pattern. Individuals with the DD pattern have the highest frequency of angiotensin-converting enzymes in their muscles. These individuals tend to have more fast-twitch muscle fibers. (2)
ACTN3
ACTN3 instructs cells to create alpha-actinin-3, a protein frequently found in fast-twitch muscle fibers. (2)
If an individual has a variant of ACTN3 known as R577X, then their alpha-actinin-3 is quickly broken down, resulting in less fast-twitch muscle fibers. If an individual is homozygous for that trait (R577XX), then they have no alpha-actinin-3 whatsoever in their muscle fibers. This leads to an individual having far more slow-twitch muscle fibers than fast-twitch muscle fibers. (6)
How Prevalent are These Traits?
Frequency of ACE D allele:
66% of Asians, 59% of Nigerians, 70% of African Americans, 46-58% of Caucasians, 33-35% of Japanese, 29% of Chinese, 15% of Yanomami Indians, and 9% of Samoans have one or more ACE D alleles. (1)
Frequency of R577X allele:
>25% of Asians, <1% of Bantu Africans, ~18% of Europeans have one or more R577X alleles.
ACE functions mainly in regulating blood pressure. It is most commonly produced by cells in the lungs, blood vessels and kidneys. (7)
It is not yet understood how variations in ACE affect athletic performance. However, there is definitely a link between blood pressure and athletic performance, so it is not surprising that ACE has an impact on athletes.
ACTN3 functions mainly in muscle fibers. It is most found in skeletal muscle. (2)
It makes sense that variations in the length of alpha-actinin-3 proteins affect athletic performance because the shorter proteins are more easily broken down, leading to a lower proportion of fast-twitch muscles.
Why get tested?
A test may be useful in order to determine what sort of muscle fibers make up an individual’s skeletal muscle and therefore what sort of athletic events they have more potential for success in.
What sort of test would be best?
A Single Gene DNA Sequencing Test that looks at either the ACE gene of the ACTN3 gene is the best option. Many tests are available that select a few key genes and examine them.
Potential options:
Atlas Sports Genetics, a company based in Colorado offers a test for $149 to determine the level of alpha-actinin-3 in an individual’s muscles. (4)
The Atlas Sports Genetics Test on amazon.com
American International offers a $200 test that looks for variations in seven genes including ACTN3 that supposedly affect an individuals’ strength and endurance. (8)
How good is the evidence?
There is little evidence linking those with the ACE DD genotype to successful speed/power athletes, and the connection between the two groups is not yet understood completely. (2)
There is strong evidence showing that high-level speed/power athletes are more likely to have the R577RR genotype while high-level endurance athletes are more likely to have the R577XX genotype. However, there are plenty of examples of successful athletes in either group who do not have those genotypes, so many more factors influence strong athletic performance. (9)
Are individuals with the trait at risk?
If an individual has the ACE DD genotype then they are at risk of developing hypertension or left ventricular hypertrophy. (7)
The ACTN3 gene does not have any major risks associated with it.
Thoughts before being tested
One should consider the multitude of factors that influence someone’s athletic potential. There are so many things that affect how one performs on a physical level, much less an emotional level. As a result, one should be aware that even if the test recommends an individual for endurance sports, it doesn’t mean that that individual with necessarily be able to succeed in those events. (3)
Reasons not to get tested
Someone should not take the test if they are planning on making decisions about whether or not to compete in a certain sport, because the test in no way indicates whether or not someone will be successful, it just points out whether one has the potential to succeed.
Ethics
Taking a test to determine what variations one has of the ACE and ACTN3 genes may emotionally impact an individual if it leads that individual to believe that they either stand no chance at succeeding in a sport or stand no chance at failing in a sport. This may lead to emotional trauma. It also may lead to parents treating their children differently as a result of a child’s genotype.
Children should not be placed in different sports just due to their genotypes
Privacy concerns?
The consumer doesn’t really have to worry about companies selling their information because it doesn’t benefit the company or harm the consumer in any way. However, they may want to consider coaches treating athletes differently due to the outcome of the test, whether that is giving them more or less playing time/attention, or even a scholarship. In addition, parents may also treat their children differently or force them to play different sports. (5)
Potential downsides
Individuals may become either apathetic or overconfident as a result of test results, and may even give up on an activity due to their genetic variations.
How do people respond to the test?
There are not any studies done on how people respond to the knowledge because it isn’t generally in the interest of the companies to see how parents react to the results.
Pre-Test Considerations
Runs in the family?
The vast majority of the tests that are currently offered look at the level of alpha-actinin-3 in an individual rather than the individual’s genotype, and variation in the ACTN3 gene only accounts for a small percentage of variation in muscle composition, so one family member’s will not necessarily predict the results of another family member’s test. (3)
How to respond to the test
An individual shouldn’t decide what sports they or their children play based on the results of the test, but it may be worth trying new things that the test claims one might be good at.
Tell a doctor?
There is no reason to tell your doctor about your results if you take a test based on the ACTN3 gene because variations in the gene don’t lead to any risks. However, one should tell a doctor if a test reveals that you are ACE DD because of the heightened risks of hypertension and left ventricular hypertrophy.
Further actions
No screenings are necessary because the test does not reveal any health conditions and should not lead one to drastically alter their lifestyle unless one has the ACE DD variation in which case one should have their blood pressure monitored.
Sources
Al-Hinai et al. “Genotypes and Allele Frequency of Angiotensin-Converting Enzyme (ACE) Insertion/Deletion Polymorphism among Omanis.” U.S. National Library of Medicine – National Center for Biotechnology Information, Apr. 2002, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3174717/
Pickering, Craig, and Kiely, John. “ACTN3: More Than Just a Gene for Speed.” U.S. National Library of Medicine – National Center for Biotechnology Information, 18 Dec. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5741991/
Rana et “al. “Association of DD Genotype of Angiotensin-Converting Enzyme Gene (I/D) Polymorphism with Hypertension among a North Indian Population.” U.S. National Library of Medicine – National Center for Biotechnology Information, 2 Aug. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5752652/
Yang et al. “ACTN3 Genotype is Associated with Human Elite Athletic Performance.” U.S. National Library of Medicine – National Center for Biotechnology Information, 3 Jul. 2003, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1180686/
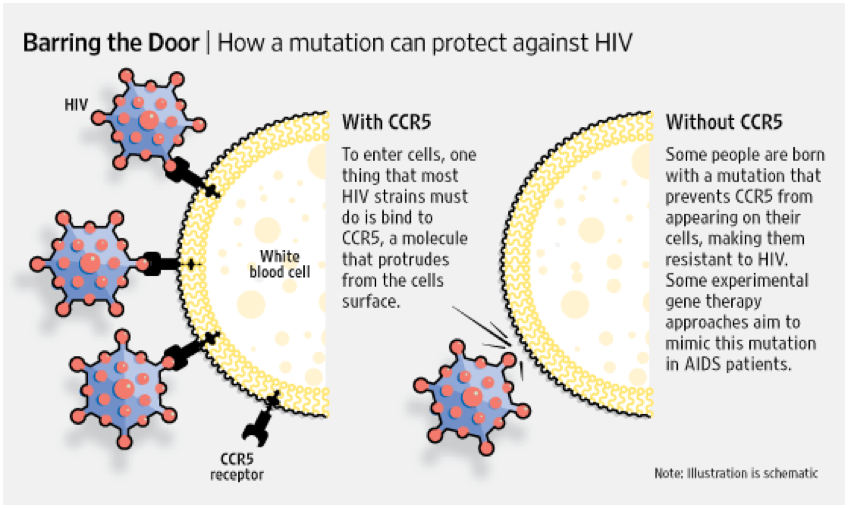
HIV is a virus that attacks your immune system. More specifically it attacks your body’s white blood cells, which are responsible for fighting off diseases. It is a sexually transmitted disease and can also common contracted through the sharing of dirty needles and from mothers during pregnancy (HIV/AIDS). Nowadays many people who have HIV can lead long lives with extensive treatment and management. However, it can still be a terrifying disease with no cure.
(Walker)
What is Delta 32?
Rs333 or CCR5 Delta32 is in the CCR5 gene which helps with many immune-related functions. More specifically it is found in the cell membrane and allows chemokines into the cell. The rs333 allele is a 32-nucleotide deletion located in chromosome 3. This alleles’ main effect is increased resistance to HIV. The allele stops the virus from being able to enter the cell. People who have one copy of this allele are somewhat resistant to the virus and the virus progresses slower. People with 2 copies of the allele are almost completely resistant to the virus. However, having 2 copies of the allele is quite rare. Only about 1% of Caucasians have this variation. It is thought this allele may have evolved in Europeans because it may have also caused resistance to the plague or smallpox. On the other hand, this allele can increase the risk of aneurysms (“rs333”).
Are there other genes that can cause resistance to HIV?
Yes, although Delta 32 is the most famous. Some genes like HLA-B57 and HLA-B27 suppress the virus’s ability to replicate. It is estimated that 3% of the population may have these alleles. Another gene known as DRB1 and DQB1 has been known to stop HIV from progressing to AIDS (PALFIR Genetics). Despite being the most well known and most researched allele linked to fighting HIV there are others that can also help your body fight the virus. Some tests, which are discussed later, that test for the Delta 32 allele will also test for these variations.
How can Delta 32 be used as a treatment?
New treatment for HIV has been built on how this allele functions. By taking medicine that binds with the co-receptor on the cell. The HIV virus is unable to bind with the cell blocking it from entering the cell (PALFIR Genetics). Some scientists have also tried to give bone marrow transplants to patients with HIV from people who are homozygous for the Delta 32 allele (Rothenberger). At this time there seem to be mixed results on the effectiveness of these transplants. Current research indicates that the use of bone marrow transplants used in tandem with other forms of treatment leads to a greater chance of fighting HIV and bringing levels of the disease in the system to below testable levels (Rothenberger).
Another case that has made international news recently is the CRISPER baby scandal. A Chinese doctor named He Jiankui edited the genes of two babies to give them the Delta 32 allele. During his testing, he failed to adhere to multiple safety protocols and has since been fired and is facing criminal investigation (Cohen). Some people have also expressed concern that without fully understanding the effects of this allele we should not be thrusting it onto babies unable to comply.
Should you get tested for Delta 32?
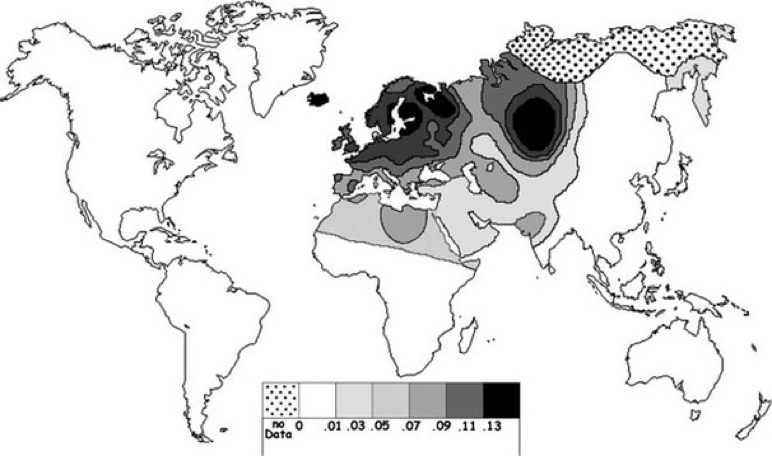
23-and-me tests for the allele but there are other companies like PALFIR Genetics that will also test for just this allele. The delta-32 specific test cost about $200 (PALFIR Genetics). At this point, there does not seem to be a good reason to get tested for this allele, especially for this cost. Since this allele is found mainly in Europeans it may be a waste of money for someone who has no European ancestors (Solloch).
(Chart showing the prevalence of the Delta 32 Allele (Solloch).)
The test may bring someone peace of mind to know they have a resistance to this virus if they have been exposed to it. However, if someone knows they are going to be exposed to the HIV virus there are other medications such as PrEP that can also lower your chances of getting the virus. PrEP is also covered by many insurance companies and can even be purchased for a discounted price if you do not have medical insurance (“Pre-Exposure Prophylaxis (PrEP)”). So instead of spending $200 to find out if you are one of the 1% who is resistant to HIV you ask your doctor about getting a medicine like PrEp instead and save a lot of money and also guarantee the outcome of lower your risk to getting the virus.
If on the other hand, you want to know if you have the allele so you can contribute to research surrounding it such as the bone marrow test or a longitudinal study about the lives of people with the allele then obviously getting tested would be the first step. Another potential problem with getting tested for this allele may be a false sense of security. Although the allele does confer almost immunity to the HIV disease and likely the plague and smallpox this does not mean people should still not be careful. At the end of the day getting tested for a genetic mutation is up to each individual and as fascinating as it sounds that your genes may make you resistant to certain potentially deadly viruses getting tested for these alleles may be more of a hassle than they are worth. I would recommend looking into some gene testing for mutations that could be potentially harmful not one that may be beneficial.
Works Cited
Cohen, Jon, et al. “The Untold Story of the ‘Circle of Trust’ behind the World’s First Gene-Edited Babies.” Science, 2 Aug. 2019, www.sciencemag.org/news/2019/08/untold-story-circle-trust-behind-world-s-first-gene-edited-babies.
“HIV/AIDS | HIV | HIV Symptoms | AIDS.” MedlinePlus, U.S. National Library of Medicine, 27 Nov. 2019, medlineplus.gov/hivaids.html#cat_77.
PALFIR Genetics. “Get Tested Now.” Are You Resistant To HIV?, 2018, www.delta-32.com/ccr5-delta32.html.
“Pre-Exposure Prophylaxis (PrEP).” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 8 Nov. 2019, www.cdc.gov/hiv/risk/prep/index.html.
Rothenberger, Meghan, et al. “Transplantation of CCR5∆32 Homozygous Umbilical Cord Blood in a Child With Acute Lymphoblastic Leukemia and Perinatally Acquired HIV Infection.” Open Forum Infectious Diseases, Oxford University Press, 22 May 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5965100/.
“rs333.” SNPedia, 3 July 2019, www.snpedia.com/index.php/Rs333.
Solloch, Ute V., et al. “Frequencies of Gene Variant CCR5-Δ32 in 87 Countries Based on next-Generation Sequencing of 1.3 Million Individuals Sampled from 3 National DKMS Donor Centers.” Human Immunology, Elsevier, 5 Oct. 2017, www.sciencedirect.com/science/article/pii/S0198885917305104.
Walker, Nick. “Umbilical Cord Blood Bank to Fight HIV and AIDS.” Umbilical Cord Blood | Parents’ Guide to Cord Blood, 2016, parentsguidecordblood.org/en/news/umbilical-cord-blood-bank-fight-hiv-and-aids.
Schizophrenia is a mental disorder characterized by symptoms including hallucinations, delusions, thought disorders and movement disorders. People with schizophrenia may also experience reduced positive emotions, and difficulty focusing. Scientists believe that schizophrenia can be both inherited and caused by the environment around an individual. Schizophrenia is typically begins between the ages of 16 and 30 and is more common in males than females. Approximately 0.4% of the population experience this genetic trait.
What Causes Schizophrenia?
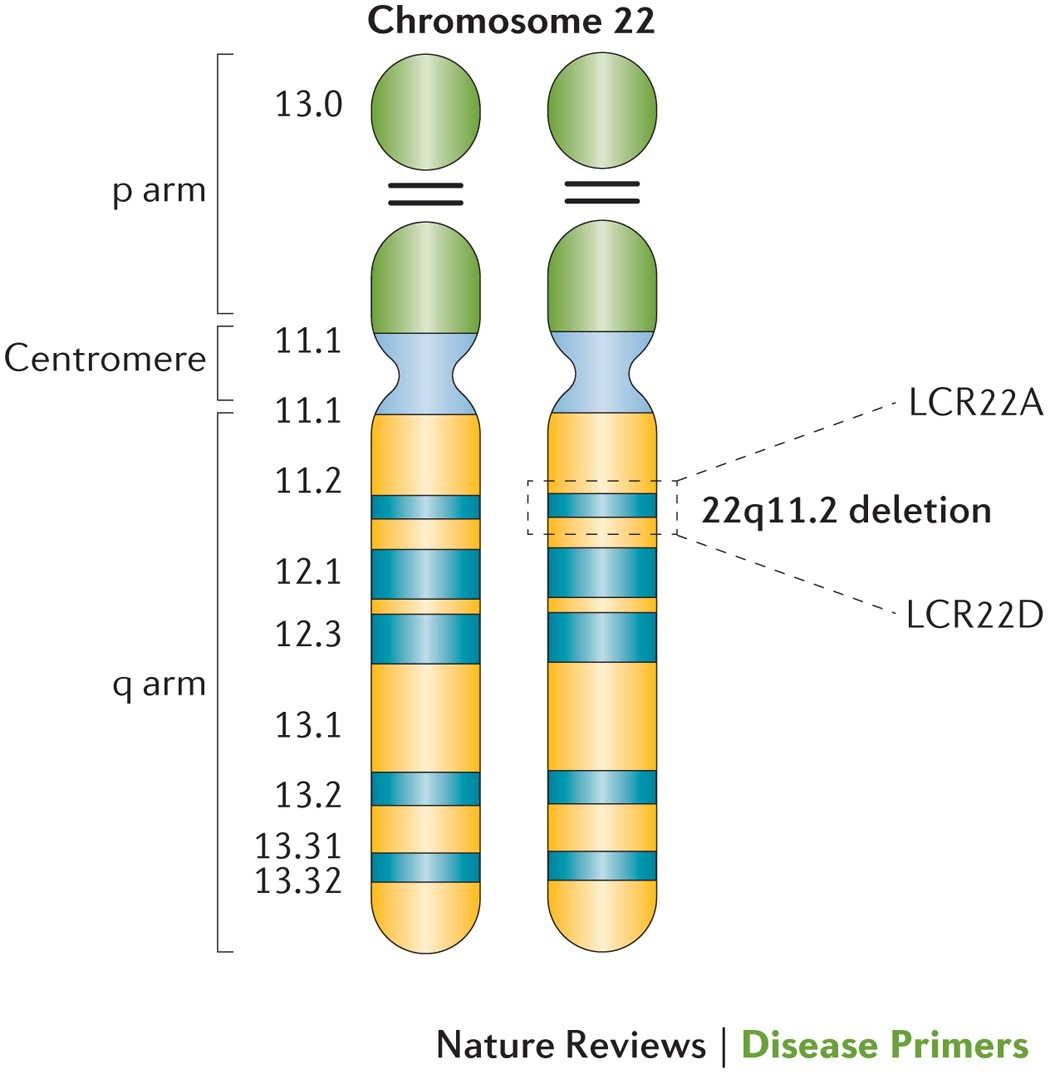
Scientists believe that many different genes can contribute to the possibility of an individual developing schizophrenia. Some studies have put the number as high as 22,000 different genes contributing to the development of schizophrenia. A microdeletion in chromosome 22 called 22q11 has been identified as most commonly linked to schizophrenia. Because of the sheer number of different genes scientists suspect increase the risk of schizophrenia, I will focus on the 22q11 mutation. This mutation deletes between 30 and 40 genes in the middle of chromosome 22.
One of the genes that is typically deleted by this mutation is the COMT gene. This gene codes for an enzyme called catechol-O-methyltransferase which is found in the brain, liver, kidneys and blood. In the brain, the enzyme helps control certain hormones and is typically found in the prefrontal cortex. The prefrontal cortex is involved with personality, planning, behavior, abstract thinking, emotion and memory. The enzyme helps maintain sufficient levels of other neurotransmitters in the prefrontal cortex which affect the abilities above.
When this gene is deleted by the 22q11 mutation it affects the production of the enzyme in the brain. The loss of this enzyme affects the ability to maintain the levels of the neurotransmitters in the prefrontal cortex. This can affect the functions of this portion of the brain.
Another gene deleted by the mutation is the TBX1 gene. This gene is responsible for the formation of tissue and organs in embryonic development. The proteins created by this gene are specifically used for development of muscles and bones in the face and neck.
When this gene is deleted by the 22q11 mutation is affects the production of the proteins. While this can cause visible changes and other medical conditions it is believed that the loss of this gene also affects behavior.
Genetic Testing for Schizophrenia
A person may want to get a genetic test because it will help them understand if they are at a higher risk for schizophrenia. Because of the number of genes thought to affect the probability of getting schizophrenia there are no tests that can accurately examine all the variables. The best option is to have a full genome sequencing because it will best be able to identify all the genes in question. However, this costs approximately $1325. A more cost effective option would be single gene sequencing. In single gene sequencing a person could examine the most common alleles causing schizophrenia such as COMT and TBX1.
Conclusiveness of Genetic Testing
There is evidence supporting a connection between these mutations and having schizophrenia. However, solely having these mutations does not mean a person will have schizophrenia. There are many different genes at play in this condition, but having these mutation will increase the chance.
Most people who have a family member who have schizophrenia will not have the condition. However, their chances are elevated compared to the average. There is no known inheritance pattern or measurable likelihood of having the condition.
Approximately 0.4% of the population have schizophrenia. Approximately 1% of people who have schizophrenia have the 22q11 deletion. Therefore if you have the variation you have a slightly elevated risk of developing schizophrenia.
Pros and Cons of Genetic Testing
Only 0.4% of the population have schizophrenia so the odds of a person having the condition are quite low. If a person has a history of schizophrenia it may be worth it to get the test done. People with a history of the condition in their family are more likely to have the disease than others. However, if there is no history of schizophrenia in your family the odds are even lower. Additionally, there are numerous variations that can cause the condition so even if the genetic test for the 22q11 deletion comes back negative a person may still have a risk of getting the condition. Also, even if a person does test positive for having the 22q11 deletion mutation they are not guaranteed to have schizophrenia it may only increase their chances.
If a person gets the test they may be fooled by the results. For example, if the person gets results that say that they have the mutation they may be worried about getting schizophrenia. However, even if they have this mutation they only have a 25% chance of having the condition. This may cause unnecessary worrying by the individual who has the test. In addition, there are many different genes which contribute to the probability of having the condition so one genetic test cannot give the individual accurate knowledge of their risk of having the condition.
The consumer may also have to worry about genetic privacy concerns. Some companies that conduct genetic testing may sell the results or may be susceptible to hacking which will jeopardize the privacy of the results. If the results are leaked the consumer may worry about discrimination in the workplace if the employer has access to the results.
Studies on Schizophrenia and Genetic Testing
There was one study that I could find on how people
react to knowing their genetic likelihood of having schizophrenia. In this
study it was found that people who were genetically more likely to have the
condition often told people about their diagnoses and some people were even
considering telling their employer.
If a person tests positive or negative they should not overreact. Neither positive nor negative test results are conclusive. If a person tests positive they may want to be conscious of the symptoms of schizophrenia. Then they could be conscious of whether they are feeling the effects of the condition and take measures to prevent it from progressing too far. Also if a person tests positive they could take steps to avoid certain activities that may put them more at risk for developing the condition. The best ways to avoid the development of schizophrenia is avoiding drugs (including alcohol) and socializing with others.
It would be helpful to tell a doctor if you have an increased risk of schizophrenia because the doctor can look out for symptoms of the condition. Often a person who has schizophrenia will not be in a good mental state so they may not voluntarily tell their doctor of their altered mental state. If the doctor knows that their patient is at higher risk of the disorder they may be more likely to notice any psychological changes.
If a person tests positive they should have psychological testing done. This will help them understand if they do have the condition and what to look out for within their mental state.
If a person thinks they are at a higher risk for developing schizophrenia they can make some efforts to lower those risks. They should avoid drugs and not overindulge on alcohol. In addition, they should try to be social and gain a positive perspective on the world. Doing these things will reduce the chances that a person develops schizophrenia.
Lawrence, Ryan
E., et al.”Concerns about Genetic Testing for Schizophrenia among Young Adults
at Clinical High Risk for Psychosis”. HHS Public Access. Jan 2017. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4982510/
Gejman, PV, Sanders, AR, and Duan, J. “The Role of Genetics in the Etiology of Schizophrenia”. HHS Public Access. March 2011. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2826121/
Schizophrenia is a mental disorder that causes a person affected by it to have a difficult time determining a difference in reality from delusions. Sufferers of schizophrenia have numerous mental struggles including delusions, hallucinations, disorganized thinking and speech, abnormal motor behaviors, and lack of proper self-care or emotion (3). Schizophrenia is not very prevalent in the human population, with only about a 1% of the world population diagnosed in the world and 1.2% of the United States population diagnosed (5). There have been numerous studies conducted regarding Schizophrenia, and it’s genetic components, but the amount of SNPs that have been believed to be associated with the mental disorder is through the roof. More recent studies have linked variations in approximately 20,000 different SNPs that influence the development of Schizophrenia (6). Other genetically related diseases typically do not have such a broad SNP range.
A recent study has determined that the SNPs rs13194504 and rs210133 have an impact on the development of schizophrenia. More specifically, the signal found between these two SNPs is what could be the culprit. The C4A and C4B alleles found in this region can form different structures among different humans creating varying amounts of C4A expression in a person’s genome. Researchers determined that a higher risk of Schizophrenia is related to a greater expression of this C4A allele, and a maximum relative risk documented at this time is 1.27. The reason is because C4A expression deals with synaptic pruning in the brain (6). Synaptic pruning is the natural removal of synapses, structures that allow the transmission of neural signals, from the brain. Pruning of the brain typically begins during early childhood and lasts into late teens or early adulthood (1). With excessive pruning, those with schizophrenia have less synapses in their brains compared to those without schizophrenia. With schizophrenia being a neurological disorder, the reduction in neural connections makes sense as to why those diagnosed with schizophrenia have such abnormal and delusional mental processes. Another factor that makes sense, the timeline of typical schizophrenia diagnoses occurring around adolescences, which would be about the same time the excessive synaptic pruning becomes noticeable.
(2)
(8)
With so many factors that influence Schizophrenia, is it really worth it to get genetically tested for Schizophrenia? In my opinion, no. The reason is that there is not a specific gene, or even 100 specific genes, that are widely recognized as the contributor to Schizophrenia. As stated above, there are over 20,000 SNPs that have variations believed to contribute to development of schizophrenia. Now, if someone were to insist they be tested I would suggest a few methods based on how much information they are looking for. If they want to know if they have even the tiniest variation in any of the SNPs associated with Schizophrenia, then I would have to tell them they need a whole genome sequence done. As of 2014, this will cost approximately $1325. With this done then the person has access to all of their SNPs, including all 20,000 that have previously been correlated to Schizophrenia development, but this will most likely be of little value to the average person. My best recommendation for those who do not want to an entire genome sequence done would be to have specific testing done on the most prevalent genes such as the structure of the C4A allele mentioned above. The Human Exome consortium has developed and is still improving a schizophrenia-oriented SNP chips based on genomes of those previously diagnosed with schizophrenia. These chips test a handful of SNPs commonly linked to Schizophrenia. A SNP chip typically costs around $300, which is much more reasonable. Again, genetic testing may not share a lot of information as the cause of this mental disorder has so much variation, so most testing is not reliable when it comes to determining the schizophrenia trait.
Scientifically, taking genetic tests
to try and determine this are not very reliable and useful. For example, just because someone has more
or less C4A alleles than someone else does not necessarily mean that they will
have significant synaptic pruning to cause neurological problems. The Indiana University School of Medicine
wrote an article regarding their new test that may predict risks of
schizophrenia. The test measures your
C4A allele and the synapses in a persons brain and uses it to determine a
possibility of schizophrenia, but even the scientists studying stated, “…[the
test] doesn’t determine your destiny. It just means that your neuronal
connectivity is different, which could make you more creative, or more prone to
illness.” (4). This statement is the
pure definition of genetic test results: unknown. Just because someone has more or less
synapses in their brain that does not necessarily mean it is going to be a
negative effect. Everyone has brain
variation, and only 1% of the population actually has schizophrenia. This test may cause unnecessary stress in a person’s
life if they are found to have a certain allele that may cause problems,
or the have a few less synapses than the person next to them. On the other hand, Schizophrenia is so
mysterious genetically that just because they appear to have a “clean genetic
health” a person could still develop a disease such as Schizophrenia.
Emotionally, genetic testing,
especially for something as serious as schizophrenia, is most likely just going
to cause unnecessary stress in someone’s life should they test positive. The Genetics Home Reference explains that
most risks that do come from genetic testing are related to emotional, social,
and financial outcomes (9). A major
issue that is often not thought about is how genetic testing affects other
members of the family. If a parent of
multiple children has schizophrenia and one child wants to be tested while
another does not this could cause issues after results are received. If the results come back with bad news, this
could cause tension and stress in the life of the sibling who did not want to
be tested. They know their sibling has higher risks, therefore they might as
well (9). There are also ethical concerns regarding the publication of research
and the right to personal health privacy through genetic testing. There are currently no “safeguards” on
sharing data from patients (7). Also, if
one family member is willing to share genetic information while another is not,
who wins the battle? This major issue
arises more frequently than not, and there are numerous debates on the
importance of sharing genetic data while also protecting a patient and his/her
family (7).
With that being said, family history
is a major factor that determines a person’s decision to get genetically tested
for certain diseases. The reason I chose
to research Schizophrenia is because my great grandmother suffered from
psychosis and I believe was eventually diagnosed with Schizophrenia. Growing up I did not know this about her and
did not find out until years after her passing.
This sparked my interest in the disease as if genetically linked I could
carry the gene. According to
Schizophrenia.com, the base risk for this gene is 1%, but with one diagnosed
parent, the offspring has a 10% chance of inheriting the disease. As someone who has schizophrenia in the
family, I still feel as though 10% is fairly low, and since it has not been
seen in generations since I feel the need to get tested is not necessary. I also feel this because schizophrenia is so
difficult to read genetically. If this
were another disease that is much easier to determine based on genetics, then
it might be a different story. I would recommend
to those who believe they are at risk to diagnose and treat as early as
possible. Seeking psychiatric services will
allow for an early diagnosis which allows for an early treatment. Medications and therapy allow those who
suffer from schizophrenia to manage their symptoms and live close to normal
lives (3).
Should a person choose to get tested, they must prepare for their results, and remember to take both a positive and a negative with a grain of salt, as results could still be inaccurate. If tested positive, or more likely to develop, a person should consult with their doctor regarding medications, treatments, stress management techniques, etc. so they are prepared and ready to battle schizophrenic effects should they arise. A few environmental factors should be taken into consideration such as decreasing use of hallucinogenic drugs such as cannabis, as well as refraining from stressful activities. Other than that, it is recommended to go on living life as usual because as said before, genetic testing for this disease is unreliable.
All in all, Schizophrenia is one of the trickiest genetic diseases to study and test. It has so many different genetic and environmental factors that makes the process of determining genetic likelihood and even diagnoses difficult. Hopefully, in years to come we can find a more definite genetic test or cause of this mental disorder, so there are less questions. For now, our society will have to continue researching and working towards finding clearer answers while understanding the ineffectiveness and unreliability that comes with genetic testing for Schizophrenia.
Sources
(1) Cafasso, J. (2018, January 3). Healthline: What Is Synaptic Pruning? Retrieved from https://www.healthline.com/health/synaptic-pruning.
(2) Hickman, R. J. (2019, August 6). An Overview of Schizophrenia. Retrieved from https://www.verywellmind.com/schizophrenia-what-you-need-to-know-4156588.
(3) Mayo Clinic. (2018, April 10). Schizophrenia. Retrieved from https://www.mayoclinic.org/diseases-conditions/schizophrenia/symptoms-causes/syc-20354443.
(4) Rattue, G. (2012, May 19). Genetic Test May Predict Risk Of Schizophrenia. Retrieved from https://www.medicalnewstoday.com/articles/245591.php#2.
(5) Recovery Brands, LLC. (2019). Schizophrenia Symptoms, Patterns and Statistics and Patterns. Retrieved from https://www.mentalhelp.net/schizophrenia/statistics/.
(6) SNPedia. (2017, October 20). Schizophrenia. Retrieved from https://www.snpedia.com/index.php/Schizophrenia.
(7) Takashima, K., Maru, Y., Mori, S., Mano, H., Noda, T., & Muto, K. (2018, June 18). Ethical concerns on sharing genomic data including patients’ family members. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6006763/.
(8) The Infographics Show. (2019, March 24). Why Do People With Schizophrenia See Things (Schizophrenia Explained)? Retrieved from https://www.youtube.com/watch?v=MN3BpNT8xqc.
(9) What are the risks and limitations of genetic testing? – Genetics Home Reference – NIH. (2019, November 26). Retrieved from https://ghr.nlm.nih.gov/primer/testing/riskslimitations.















{kind=link}
{kind=link}
{kind=link}