Alcoholism, which can also be called alcohol use disorder, affects an estimated 14.1 million adults in the United States (1). It has been linked to different SNPs in 6 main genes, all of which have to do with chemicals or hormones in the brain. OPRM1 and DRD2 are receptors for opioids and dopamine, respectively, while SLC6A3 and SLC6A4 are transporters of dopamine and serotonin. GABRA2 is a GABA receptor gene, and GABA is an inhibitory neurotransmitter. GHSR is the gene that is a receptor for growth hormones (2). The genes linked to alcoholism have to do with the chemical balance of the brain, because imbalance of those chemicals can lead to psychiatric disorders, such as alcoholism. While a person cannot be completely confident that they will develop alcoholism based on the presence of these genes, the genetic predisposition to alcoholism may be a reason to take preventative measures.
To test for alcoholism, I would
recommend a SNP chip. If there were a chip with the SNPs that are implicated in
the tendency towards alcoholism, it would only cost $300 to determine whether a
person has a tendency towards alcoholism. A person may want to get this test if
they are concerned about the development of alcoholism in their future. If they
get the test, they can make the decision to be proactive about how much alcohol
they consume. However, even if the tests are positive, it does not mean that
they will definitely develop the disorder; it simply means they are at higher
risk because the mutations in their genes make a person more likely to have
alcoholism.
Additionally, the studies on some of the SNPs that are considered to be linked to alcoholism have had mixed results. This means that we are not completely sure of the association between the SNP and alcoholism, so there are significant limitations to the degree to which the genetic tests can predict a person’s likelihood of developing alcoholism. Other variants such as the environment that a person lives/grew up in, may impact the likelihood of developing alcoholism as well, and those cannot be predicted by a genetic test (4). If someone tests positive for most of the SNPs that are associated with alcoholism, then they are at a higher risk for developing the disease. However, this still is not a guarantee of them getting it. Any lifestyle changes that a person chooses to implement based on positive results of the genetic tests may be completely unnecessary, and the person would have disrupted their life out of fear of a disease that they may never develop (5).
There is still some debate as to whether alcoholism is
genetic or hereditary. If someone in the family has already tested positive for
the SNPs that are associated with alcoholism, other members of the family may
be at higher risk and should consider getting tested if they are worried about
developing the disease; however, this is not a guaranteed correlation. If a
person does test positive for the associated SNPs, they should monitor their
alcohol consumption carefully, and perhaps ask a trusted friend or family
member to keep them accountable. If the person wants to take prevention very
seriously, or if they have had issues with addiction in the past, they could
give up the drug altogether. The person should share the results of the test
with their doctor in order that their doctor can make decisions regarding
treatment plans with addictive medications, because addition to alcohol is
often associated with other addictions.
Overall, people who are very
concerned about the possibility of developing alcoholism in their future could
complete a genetic test that shows whether they have SNPs in their genes that
are consistent with those linked to alcoholism. However, they must bear in mind
that even if they undergo the genetic testing and test positively, they may not
develop the disease, and vice versa. Genetic testing for alcoholism has its
limits, and one cannot take the test and expect its results to be a guarantee
of whether or not they will develop the disease.
“Alcohol Facts And Statistics.” National Institute On Alcohol Abuse And Alcoholism (NIAAA), https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-facts-and-statistics. Accessed 4 Dec. 2019.
“Is Alcoholism Hereditary Or Genetic?” American Addiction
Centers, https://americanaddictioncenters.org/alcoholism-treatment/symptoms-and-signs/hereditary-or-genetic.
Accessed 4 Dec. 2019.
“What Are The Risks And Limitations Of Genetic Testing?”
Genetics Home Reference,
https://ghr.nlm.nih.gov/primer/testing/riskslimitations. Accessed 4 Dec. 2019.
With the rising uproar over speculations that vaccines cause Autism, there is a need to look into the causes of autism, especially to indicate that there is no credible evidence that indicated an actual connection between vaccines and the cause of Autism.
What is Autism?
In modern days, Autism is actually referred to as Autism
Spectrum Disorder. Autism Spectrum Disorder is described by NIMH as a
developmental disorder that affects communication skills and behavior.1
This change in the name is due to the fact that the symptoms of Autism span
over a spectrum. Therefore, symptoms are specific to each individual. However,
there is still a set criterion used to diagnose the disorder, which are outlined
in the DSM-5. These diagnostic criteria fall into five different categories: reoccurring
lack of social skills (such as communication and interaction) in multiple scenarios,
restrictive and repetitive acts of behavior, symptoms must be present in early
childhood or developmental stages, symptoms must cause clinical impairment in the
functioning of areas of one’s daily life,
and lastly these impairments must not be better explained through other intellectual
disabilities or developmental delay.2
In the US, it was determined that there are approximately 1
out of 59 children diagnosed with this disability during 2018.3
Genetic Relevance?
According to Genetics Home Reference, there are at least
1000 genes that are associated with the disorder, but not all of them have been
confirmed (none of which are listed).4 Most of these associated
genes (left unnamed in the article) have little effect in causing the disorder.4
The specifics of the effects of these genes are not listed; however, it is
known that the probability of these mutations combined together and with other
risk factors, the risk of autism can be calculated. Therefore, autism is not
cause entirely by genetic factors alone.
Other associated genes mutations are rare and happen in a
single gene. One such genes is ADNP, which also causes ADNP syndrome (another intellectual
disability).4 The syndrome has additional conditions to Autism
Spectrum Disorder. Another set of genes associated with Autism Spectrum Disorder
are ARID1B, ASH1L, CHD2, CHD8, DYRK1A, POGZ, SHANK3, and SYNGAP1.4 Most
of these mutations are used for brain development.4 Another gene that
has a significant effect on the development of Autism is rs1858830.5
The allele for G;G codes for normal genes.6 However, the allele C;G
is known to increase the risk of Autism development by 1.6, and the allele C;C
is reported to increase the risk of Autism development by 2 fold.6 The
specifics of how these mutations affect brain development is unknown.
Testing?
There has been a study that connected abnormalities of
certain genes to the development of autism.7 This study recommends
taking genetic testing as a precaution, given that not every family would
follow the advice.7 However, other studies do not recommend using
genetic tests as a method of diagnosis and even detection.
Similar to the other studies, the CDC (Centers for Disease
Control and Prevention) does not include any medical testing (such as a blood
test) as a method of diagnosis.8 Instead they use behavioral and
developmental cues through developmental screening and comprehensive diagnostic
evaluation.8
Despite genetic testing for Autism being possible, there is no actual test provided by companies.
It is important to note that since autism is a behavioral disorder, it is hard to diagnose through physical tests, such as genetic tests and blood tests. This does not mean testing is waste a time per se. These tests can determine the probability of a person developing autism; therefore, genetic testing should be taken as a precaution but not as a diagnosis. It is advised to use developmental screenings and diagnostic evaluations to diagnose the disorder. In the end, it can be concluded that there is absolutely no connection between vaccines or the ingredients and autism.
Resources:
Autism Spectrum Disorder. National Institute of Mental Health. https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd/index.shtml. Published March 2018. Accessed December 3, 2019.
Ciccarelli SK, White JN. Psychology: DSM 5. Boston: Pearson; 2014.
Autism Facts and Figures. https://www.autismspeaks.org/autism-facts-and-figures. Accessed November 14, 2019.
ASD – Genetics Home Reference – NIH. https://ghr.nlm.nih.gov/condition/autism-spectrum-disorder. Published November 26, 2019. Accessed November 14, 2019.
Autism. https://www.snpedia.com/index.php/Autism. Published October 25, 2017. Accessed November 14, 2019.
rs1858830. SNPedia. https://www.snpedia.com/index.php/Rs1858830. Published December 1, 2018. Accessed December 3, 2019.
Çöp EM, Yurtbaşi PM, Öner ÖM, Münir KM. Genetic testing in children with autism spectrum disorders. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4560248/. Published 2015. Accessed November 14, 2019.
Screening and Diagnosis of Autism Spectrum Disorder. Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/autism/screening.html. Published August 27, 2019. Accessed December 3, 2019.
Parkinson’s disease is here and affecting many people’s lives. It’s the runner-up neurodegenerative disorder making it the second most common disease next to Alzheimer’s disease. In North America alone, more than one million people are affected by it. Parkinson’s disease is distributed among “1% of 55-year-olds and more than 3% of those over age 75”. Altogether, there are more than four million people with PD worldwide(6).
There are 18 chromosomal regions involved in Parkinson’s. However, “[not] all of the identified genes contain causative or disease-determining mutations”(4). For example, alterations in GBA and UCHL1, “do not cause Parkinson disease but appear to modify the risk of developing the condition in some families”(5). The names of the regions are numbered chronologically from PARK1 to PARK18. These names are really nick-names of the underlying regions. For example, PARK6 is really PINK1. Relating to the genes, “we know of 28 distinct chromosomal regions more or less convincingly related to PD. Only six of these specific regions contain genes with mutations that conclusively cause monogenic PD” or “a form of the disease for which a mutation in a single gene is sufficient to cause the phenotype”(4). NIH states that “variations in other genes that have not been identified probably also contribute to Parkinson’s disease risk”(5).
Specifically, “Familial cases of Parkinson’s disease can be caused by mutations in the LRRK2, PARK7, PINK1, PRKN, or SNCA gene, or by alterations in genes that have not been identified”. However, mutations of these genes can happen to people who have not inherited the disease and the causes of these sporadic mutations are unknown. The functions of all the proteins generally are producing dopamine in the “substantia nigra”(5). Therefore, these proteins are a part of dopamine-producing neuron cells and are made in these specific neuron cells. Because these genes produce proteins that produce dopamine, it makes sense that an alteration, variation, or change in the structure of these proteins would lead to a lack of dopamine production in the brain, thus leading to the trait of Parkinson’s disease.
Source: WebMD(8)
Why Get Tested?
Genetic testing for Parkinson’s disease has not been formalized under either the “Movement Disorder Society or any other PD alliance group”. Testing is encouraged for those with “juvenile-onset PD irrespective of family history; early-onset PD with atypical features and/or a positive family history of this disease; or late-onset PD with a strong family history of PD”. Genetic testing is strongly recommended for patients with early-onset PD. This is to help these people “understand their disease and to make informed life decisions”. It has been argued that testing would not change the clinical management of Parkinson’s. However, according to a journal by Christine Klein and Ana Westenberger(4) that is published on pubmed.gov, testing is becoming exceedingly more important in identifying mutations that will lead to more effective treatment routes(4). If the patient wants more effective treatments, testing is a viable option. It is important for understanding how family plays a role in PD. To start, only fifteen percent of those with PD have a family history with ten percent being reported from other sources(5). However, it is still important for those who have relatives with PD to understand how the disease spread through their family. The genes that spread through a family are the aforementioned LRRK2, PARK7, PINK1, PRKN, and SNCA genes. Furthermore, genes that affect Parkinson’s disease are (1) autosomal dominant, (2) autosomal recessive, and (3) autosomal dominant with reduced penetrance. “In clinical practice, however, pedigrees rarely follow that aforementioned well-defined Mendelian inheritance patterns, i.e., they are frequently complicated by reduced penetrance, variable expressivity, and phenocopy phenomena”(4). Because of this and the variability of inheritance patterns across the genes that lead to PD, it is important for people to be aware of family history in order to make an informed decision about testing for PD.
For those who decided to test for PD, I recommend a single-nucleotide polymorphisms test in order to determine whether you have certain variants that “are considered to be [associated] with the disease”(4). The cost to test for all six known genes would cost $4,000 and would not be covered by Medicare(1). The type of test recommended given for the most common alleles for Parkin. Parkin mutations account for “77% of the familial cases with an age of onset [less than thirty years] (Lucking et al. 2000), and for 10%–20% of patients in general”. In addition to Parkin, LRRK2 and PINK1 are more common monogenic forms in which testing is recommended. However, testing is generally discouraged for those without “juvenile-onset PD irrespective of family history; early-onset PD with atypical features and/or a positive family history of this disease; or late-onset PD with a strong family history of PD” as mentioned previously(4). Moreover, there is good evidence supporting a connection between these variations and the trait in question in cases where “many family members affected by Parkinson’s disease”(7). The base risk of PD increases with age as PD typically develops in middle to late life. After identifying the variation, the person’s actual risk is not significantly increased unless the person has a family history of the disease.
Think Before You Spit:
There are scientific reasons that someone should not test for PD. There are no diagnostic criteria for SNPs for PD and therefore should avoid testing unless PD is prominent in the family. Risks of misdiagnosis are increased when these types of tests are taken because of a lack of conclusiveness. “Because there is no conclusive screening or test, patients with very early Parkinson’s disease may not meet the clinical diagnosis criteria. On the flip side, this lack of specificity means that you could be diagnosed with Parkinson’s disease, only to find out later that you have a different condition that mimics Parkinson’s”. Instead of genetic testing, the FDA has “approved an imaging scan called the DaTscan. This technique allows doctors to see detailed pictures of the brain’s dopamine system.” Furthermore, “The results of a DaTscan can’t show that you have Parkinson’s, but they can help your doctor confirm a diagnosis or rule out a Parkinson’s mimic”(3).
Ethical Considerations:
There is always a concern for privacy when it comes to genetic testing. Our genes contain personal biological information, so it is recommended that one doesn’t get tested if (1) it’s not needed or (2) doesn’t live in a nation-state where genetic privacy rights are strongly protected. It is important that you weigh the pro and cons of getting testing especially if the testing could benefit treatment management.
Potential downsides of getting the test include (1) getting results that are not conclusive, (2) increased stress or anxiety from seeing results, and (3) getting misdiagnosed or misinformed. According to Roy Alcalay(1), an assistant professor of neurology at the Taub Institute, “positive findings may induce anxiety among first degree family members (who have a 50% chance of carrying the genetic risk as well), and a fear of discrimination (e.g. for employment or insurance purposes) based on the genetic findings”(1).
Asking the Right Questions Before Getting the
Test:
Given the large variability of inheritance, the chances that a child, nephew, or aunt will test positive is largely incalculable. Generally, it would be advantageous for one to determine if the disease is either autosomal dominant or autosomal recessive. However, this method of calculating the probability is not effective because “pedigrees rarely follow that aforementioned well-defined Mendelian inheritance patterns”(4).
Testing positive or negative is often misleading for PD. Oftentimes patients will test positive for PD and either not have or have another disease. For patients with a family history of PD, however, testing positive for PD is an indication that the patient should see a specialist and seek a guided treatment managed with consideration of the additional information from the genetic test. For patients who tested under these similar familial circumstances, but instead tested negatively, it is important that they continue to be aware of their familial risk factors and seek additional information as it becomes available.
If you get a test and would like to share the results with a doctor, it is important that you forward the information effectively. That is to inform your doctor why you got the test and what concerns you had leading up. Discuss with your doctor if there are any recommend steps or additional informative outlets about your test results.
For those who test positive, an additional DaTscan which has been approved by the FDA is recommended so that doctors can collect additional information on the dopaminergic neurons (3). While a positive test does not determine Parkinson’s disease conclusively, it is important that a patient tries to decrease other risk factors associated with the environment. “Exposure to certain toxins or environmental factors may increase the risk of later Parkinson’s disease, but the risk is relatively small”(7). In other words, it is encouraged to avoid toxins, but the effect is small compared to other risk factors that are already at play.
Works Cited
(1) Alcalay, R. N. (2016, April 15). Parkinson’s: risk factors, genetic testing and therapies. Retrieved from http://blogs.biomedcentral.com/on-medicine/2016/04/18/parkinsons-risk-factors-genetic-testing-therapies/.
(2) EurekAlertAAAS. (2007, February 22). Low-cost Parkinson’s disease diagnostic test a world first. Retrieved from https://www.eurekalert.org/pub_releases/2007-02/ra-lpd022207.php.
(3) How Parkinson’s Disease Is Diagnosed. (n.d.). Retrieved from https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/how-parkinson-disease-is-diagnosed.
(4) Klein, C., & Westenberger, A. (2012, January). Genetics of Parkinson’s disease. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3253033/.
(5) Parkinson disease – Genetics Home Reference – NIH. (n.d.). Retrieved from https://ghr.nlm.nih.gov/condition/parkinson-disease#resources.
(6) Parkinson’s disease. (n.d.). Retrieved from https://www.snpedia.com/index.php/Parkinson’s_disease.
(7) Parkinson’s disease. (2018, June 30). Retrieved from https://www.mayoclinic.org/diseases-conditions/parkinsons-disease/symptoms-causes/syc-20376055.
(8) Parkinson’s Disease: Symptoms, Causes, and Treatment. (n.d.). Retrieved from https://www.webmd.com/parkinsons-disease/ss/slideshow-parkinsons-overview.
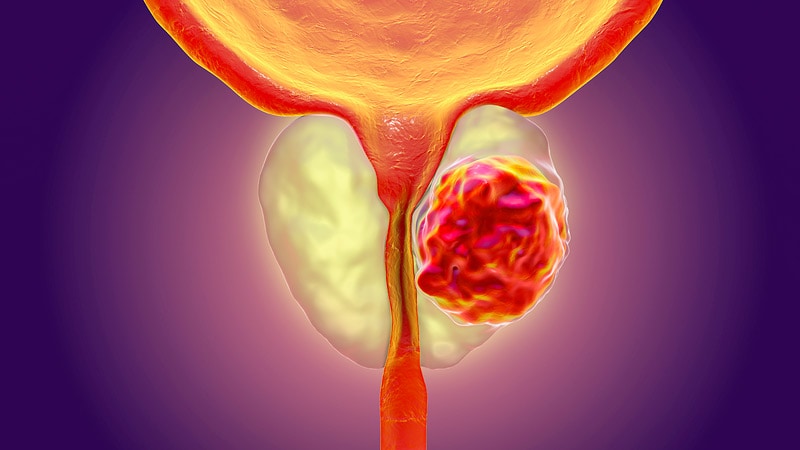
The prostate is a gland
found in male bodies that surrounds the urethra and is crucial in the
development of semen. Prostate cancer is a disease predominantly affecting
middle-aged and older men, where cells in the prostate gland multiply rapidly
and form a tumor. The disease affects about 1 in 7 men [2].
Prostate cancer can develop
at an early stage without pain, but can become fatal in later stages. Hence,
early detection is essential for men.
The Genetics
Aside from environmental factors, the form and function of our entire body is encoded in our DNA. This is a molecule contained in all of our cells, and the code, split into genes, is formed by sequences of 4 letters: A, C, T, and G. Although there are billions of these letters throughout our DNA, even a small change—or mutation—can drastically damage the human body.
Research has shown that
some of these miniscule mutations, particularly in any of 5 specific genes, are
strongly linked to prostate cancer development. There is also another gene,
called BRCA1, that helps code for proteins that suppress tumor growth. This
gene corrects mistakes that are made when duplicating our DNA, so that (in
theory) our genes stay the same over time. Put more simply, BRCA1 works to
prevent mutations—which may cause tumor growth—from occurring.
Why get tested?
With this information
alone, any man would consider getting a genetic test for prostate cancer, and
for good reason. Even having 2 of the 5 aforementioned mutations could double
your odds of developing the disease [1]! And inherited mutations (those which
are often passed down from family members) in BRCA1 and similar genes monumentally
increases cancer risk [2]. Knowing your odds is key to detecting prostate
cancer early (when it is low-risk), treating it before the tumor grows out of
control, and ultimately beating the disease.
If you’re looking for a
genetic test, try out the SNP-chip, which can detect such single-letter
mutations across different genes for around $300. But you may want to consider
the alternatives first.
Alternatives
There are many ethical issues
of genetic tests. Depending on how much of your DNA you want sequenced, the
results can tell you about untreatable and uncurable diseases. Also, many companies
will sell data and infringe on your privacy, so it is crucial to use a
reputable service.
Additionally, the genetic
test may not even be accurate. In fact, most cases of the cancer are somatic
mutations, types that occur throughout a person’s lifetime and are hence not
inherited. In this case, a genetic test can give a false sense of security.
Even family history may only account for around 50% of cases of the disease [2].
As an alternative, there are more precise tests and screenings that can detect prostate cancer at an early stage. The two most common are rectal exams and PSA tests (a specific blood test), which have proven to be accurate and recommended by doctors [3].
Personal Considerations
Family history alone can
have the same effect in increasing your odds as a single one of the above
mutations. In these cases, it may be advantageous to get a genetic test at a
young age, before the disease even starts to develop.
However, there is little danger
in waiting until your late 30s or early 40s, when prostate cancer could be at an
early stage of development to get tested. In this case, more-accurate rectal
exams and PSA screenings are recommended, especially for those with family
history.
It should be noted that
there are potential side-effects to treating (or overtreating) prostate cancer,
such as erectile dysfunction and infections [4]. In some cases, the disease can
be nonfatal and unharmful. However, since prostate cancer can likely become
fatal if not treated early, the choice of whether to take action against it is
clear. It is never too early to talk to your doctor about your risks!
Sources
[1] Zheng SL, Gelmann EP, Kearon C,
Kapur J, Center for Human Genomics. Cumulative Association of Five Genetic
Variants with Prostate Cancer: NEJM.
https://www.nejm.org/doi/full/10.1056/NEJMoa075819. Published February 28,
2008.
[2] Prostate cancer – Genetics Home
Reference – NIH. U.S. National Library of Medicine.
https://ghr.nlm.nih.gov/condition/prostate-cancer. Accessed December 3, 2019.
[3] Prostate cancer prevention and
early detection. Prostate cancer prevention and early detection | Seattle
Cancer Care Alliance.
https://www.seattlecca.org/diseases/prostate-cancer/early-detection-prevention.
Accessed December 3, 2019.
[4] What Are The Side Effects Of Prostate Cancer Treatment? Prostate Cancer Foundation. https://www.pcf.org/about-prostate-cancer/prostate-cancer-side-effects/. Accessed December 3, 2019.
Genetic genealogy is
a new forensic technique that has taken the crime-fighting world by storm. By
sending your DNA to companies such as 23andMe or AncestryDNA, you can help
catch violent criminals, mostly of unsolved murder and rape cases, and solve
cases from years ago and now. While it may be controversial, many criminal
cases have been solved and the perpetrator has been caught using this
technique. For example, the Golden State Killer, who terrorized women
throughout the state of California during the 1980s, was caught in 2018 using
genetic genealogy (1).
Is It Okay for Law Enforcement to Have Access to Consumers’ DNA?
Many
DNA databases have now allowed law enforcement access to their information
through the new terms and conditions. For a while, there was controversy
surrounding the idea of law enforcement having access to the DNA within these
databases for violent crime investigation without the consumers explicitly
being notified. A company called FamilyTreeDNA was exposed for allowing law
enforcement access to the genetic profiles of over a million users (2). Many
people thought this was an invasion of privacy, especially considering they did
not give consent for their DNA profiles to be viewed and used by law
enforcement. FamilyTreeDNA’s response to the criticism was that they felt a
moral obligation to help solve violent cases given the information they had (3).
Now, people seem to not have an issue with their DNA being available to law
enforcement, considering that many criminal cases have been solved thanks to
the use of genetic genealogy (2). Now, the concept of law enforcement having
access to consumers’ DNA is less of a controversy, as long as there is
transparency between law enforcement, the DNA database companies, and the
customers.
How Does It Work?
DNA from crime scenes
are inputted into the genetic database GEDmatch and cross-referenced with DNA
of consumers within databases like 23andMe and AncestryDNA. If a match is
found, it is most likely a distant relative of the perpetrator of the crime.
Law enforcement can then trace back through the ancestry tree to find the
person in the family who committed the crime and arrest them (1). This
technique is especially helpful for older cases, when DNA testing couldn’t be
used. The technique requires testing of
Y-DNA, which is a genetic test that follows the paternal lineage. This
increases the popularity among forensic investigators because it’s the best way
locate relatives through the male genetic line as well as determine the gender
of the person’s DNA left at the crime scene (4).
Convicting Family
The
biggest concern with this new forensic technique is that people will be
unknowingly giving information to law enforcement that could get someone in
their family convicted on a violent crime. While this seems to be a big issue,
most of the relatives found through forensic genealogy are distant relatives,
such as third or fourth cousins, and don’t even know the relative who committed
the crime (2). Many people also feel that everyone should do time for violent
crimes they have committed, such as murder or rape, even if it means helping to
put a family member in prison. While it’s easy to look at the situation from an
outside perspective and say that it is one’s moral responsibilty to give their
DNA to solve crimes, even if it means getting a family member arrested, there is
much more to consider in reality. The emotional distress that can come from
making this decision is very difficult to put upon a family member. It is also
very difficult for people to put aside family loyalties to get justice for someone
they probably don’t know.
Should You Send in
Your Spit?
Many campaigns have
come out supporting the use of forensic genealogy and advocating to the public
that they can help catch violent criminals by sending in their DNA. The most
famous advertisement is Ed Smart’s ad for the genetic testing company
FamilyTreeDNA, which advocated for allowing law enforcement access to DNA
databases and asking viewers to send in their DNA (3). Ed Smart’s daughter is
Elizabeth Smart, who was abducted when she was 14 years old. His message was
that the families of victims of violent crimes need and deserve answers, and
that your DNA could be the missing piece to finding those answers (3). I would
recommend that you send in your spit, because the possibility of solving a
violent crime with your DNA could mean giving closure to and getting justice
for a victim or a victim’s family.
Sources:
1. Corbyn, Z. (2019). How taking a home genetics test could help catch a murderer. https://www.theguardian.com/science/2018/dec/01/how-home-dna-tests-are-solving-cold-cases-golden-state-killer [Accessed 14 Nov. 2019].
2. Zhang, S. (2019). A DNA Company Wants You to Help Catch Criminals. [online] https://www.theatlantic.com/science/archive/2019/03/a-dna-company-wants-your-dna-to-catch-criminals/586120/ [Accessed 14 Nov. 2019].
3. MIT Technology Review. (2019). Help us catch killers is now the new advertising angle for DNA companies. https://www.technologyreview.com/f/613232/help-us-catch-killers-is-now-the-new-advertising-angle-for-dna-companies/ [Accessed 14 Nov. 2019].
4. Corporation, P. (2019). Forensic Genealogy: What Your Second Cousin’s DNA May Say about You – ISHI News. https://www.ishinews.com/forensic-genealogy-what-your-second-cousins-dna-may-say-about-you/ [Accessed 14 Nov. 2019].
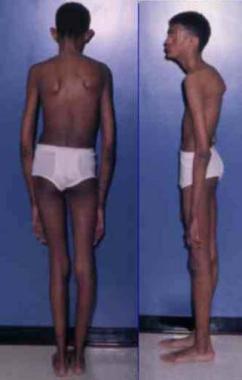
Marfan syndrome is a disease that usually causes vision problems and defects in large blood vessels from the heart. This happens because Marfan syndrome is a disease that affects connective tissues in the body. Marfan syndrome can appear at any point in an individual’s life and can be fatal if it is not treated. This disease affects roughly 1 in 5,000 people around the world and is caused by a mutation in the FBN1 gene. The gene FBN1 creates the protein fibrillin-1 which helps to form connective tissue. Fibrillin-1 creates structures called microfibrils that help connective tissue function properly. Without these microfibrils, the body will overgrow, and tissues will become unstable (5). A common symptom of Marfan syndrome is elongated limbs such as in this image:
(3)
Some signs of Marfan syndrome are elongated limbs and loose joints as well as an irregular heartbeat, shortness of breath, and general fatigue. It would be smart to get a genetic test done if you showed any of these symptoms and believed that you may have Marfan syndrome. That is because early treatment is crucial to living out a normal life with this disease. Because there is only one gene associated with the development of Marfan syndrome, I would recommend getting a single-gene sequencing done. I recommend this because there are over 1,300 mutations that could cause Marfan syndrome (2). This test will cost roughly $1,400 to $2,000 (4). The evidence between the variations found in this test and the trait are very solid. Individuals who have one of the variations in their FBN1 gene will have Marfan syndrome, although there are people who show some symptoms of Marfan syndrome but do not actually have the disease.
An issue that an individual might have if they get the test done is that their entire life could change if they find out they have the disease. If a person found out that they had the disease, they would then have to go through regular treatments and alter their lifestyle because of this disease. If a person had Marfan syndrome, it would be ideal to limit exercise and avoid any hard contact or overly strenuous activities (4). Along with lifestyle changes, the test and treatments are expensive. While these may cause someone to not get tested, this trait is inherited in an autosomal dominant manner, meaning that if either of the two alleles is mutated, the individual will have the disease (5). However, if your family has no history of the disease, then the test is not necessary unless symptoms occur.
Testing positive for Marfan syndrome would weigh heavily on a person’s conscious. As a consumer, you would want to assure that the results of the test were either sealed or anonymous to the public. Some downsides of taking the test are the cost and the emotional baggage that may come with the results. I couldn’t find a study on how people reacted to the results of their genetic testing, but individuals with Marfan syndrome came out in an article done by The Mightyand stated some things that they wish others knew about those who have the disease. One person stated that they live in “constant pain” and others motioned that the disease is not the same in every person and that there isn’t just one specific way that a person with the disease might look (1).
To make sure that testing is necessary, there are a few things that a person can check for on their own before making a decision. If one of your parents has the disease, or you begin to show symptoms, it is a very good idea to get tested. Before being tested, you should make a plan on what you will do following the results of the test. It is smart to do this beforehand because there may be disappointing results. If you test positive, you should begin treatment as soon as possible and talk to your doctor about lifestyle changes that may need to be made. In the event that you test negative, nothing needs to change.
If I tested positive, I would make sure to tell my doctor so that I would be getting the correct treatment for the disease. I would tell my doctor something along the lines of this: “Hello Dr.______, As you know, members of my family have had Marfan syndrome and encouraged me to get tested. I had a genetic test done and I tested positive for Marfan syndrome. I will begin treatments as soon as possible and I just wanted to let you know in case there are other medical issues that may arise from this. Thank You, Chad Hudak”.
The disease known as Marfan syndrome is very rare and affects very few people around the world. Because of this, it is not necessary to be worried about the disease unless you have a family history or symptoms occur. Marfan syndrome is not a life-threatening disease as long as precautions are taken to ensure good health.
Works Cited
Brentano, Elisabeth. “17 Things People With Marfan Syndrome Wish Others Understood.” The Mighty, 14 Nov. 2019, themighty.com/2015/11/living-with-marfan-syndrome-what-to-know/.
“FBN1 Gene – Genetics Home Reference – NIH.” U.S. National Library of Medicine, National Institutes of Health, 12 Nov. 2019, ghr.nlm.nih.gov/gene/FBN1.
“The Marfan Foundation.” The Marfan Foundation, www.marfan.org/.
“Marfan Syndrome – Genetics Home Reference – NIH.” U.S. National Library of Medicine, National Institutes of Health, 12 Nov. 2019, ghr.nlm.nih.gov/condition/marfan-syndrome#.
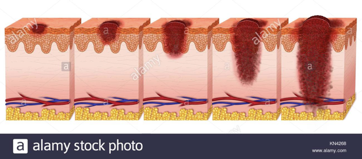
Malignant melanoma is the most serious type of skin cancer, and it is characterized by the uncontrollable growth of melanocytes (skin cells that produce melanin). In the United States, melanoma affects 30 out of 100,000 men and 18 out of 100,000 women (“Melanoma”, 2018).
The graphic above illustrates the
progression of melanoma. The disease gets more serious as it spreads deeper
into the skin. The survival rate of
melanoma at the first stage is at 98.5%, and it drops down to 22.5% at the final
stage (“Melanoma Survival Rates”, n.d).
Melanoma is a condition where a single gene doesn’t dictate the disease. However, there are many genes that are linked to the disease. Two of the main genes are CDKN2A and BAP1. A mutation of the CDKN2A is linked to greater risk of developing melanoma. (Hayward, 2003). The specific mutation of CDKN2A disrupts the proteins that function as tumor suppressants. The mutation of this gene also leads to developing melanoma at a younger age and greater risks of other cancers. With the CDKN2A mutation, you are around 28% more likely to develop melanoma (“CDKN2A”, n.d.). Another gene linked to melanoma is BAP1. A dominant inherited allele on the rs387906848 SNP causes BAP1 tumor predisposition syndrome (“rs387906848”, n.d.). This condition increases the risk of cancerous and noncancerous tumors from 14% to 29%. The BAP1 mutation also has an incidence of malignancy of around 70% (Carbone et al., 2013).
Why
Get Tested?
While genetic tests won’t say you’re set to develop melanoma, it will make you aware of certain risks associated with the disease. Because there are so many genes associated with melanoma, a single gene DNA sequence, whole genome sequence, or a SNP Chip test are recommended. Since the genes linked to melanoma are known, a test would analyze the presence or mutation associated with each gene. Companies such as AmbryGenetics, Invitae, and GeneDx offer genetic tests that will analyze genes associated with melanoma. These tests will indicate if you are more at risk to develop melanoma. When looking at tests, it is best to use one that is able to scan for multiple genes. The whole genome test, while expensive, will show your exact genetic markup. The SNP Chip test is a cheaper alternative that looks at the specific melanoma related genes. Ultimately when deciding on a test, it depends how much you want to know and how much you are willing to spend.
Think Before you Spit
One of the main reasons to not take
a test is that it won’t clearly tell you if you will develop melanoma. Around
90% of people who develop melanoma do not have a genetic mutation that accounts
for it (“Should I Get”, n.d.). Environmental factors such as UV radiation are
the main cause of melanoma. The test results may be confusing for some
consumers, and it may cause them to make irrational decisions. Therefore,
because of the limited predictive value of the tests, genetic tests for
melanoma are not worth the time and money.
There are some concerns with privacy associated with genetic testing. Some patients are concerned that genetic test results may result in discrimination by insurance providers. However there are laws such as the Genetic Information Nondiscrimination Act that helps protect patients. There are other ethical concerns associated with genetic testing. For instance, there can be liability issues associated with genetic test results. An example of this is a patient’s decision to conceive children or to terminate pregnancies based on test results (Dickens, Pei, & Taylor, 1996). Genetic tests effectively dictate the decisions people make, and some people may not fully understand the results of the test. Test results can cause stress, and they can drastically change lifestyles. There is also concern about employer discrimination associated with genetic test results.
Asking
the Right Questions Before Getting the Test
For melanoma, genetic tests aren’t the sole decider of the disease. The genetic test results will show different genes that put you at risk to develop it. For example, if someone tests positive for the BASP1 tumor predisposition syndrome, it is likely that one of their parents had the condition. This is because the syndrome is autosomal dominant. If someone tests positive for genes associated with melanoma, they should be aware of the risks. The first thing to realize is that you aren’t guaranteed to get it. If you are careful about sun exposure and annual skin screening, you can easily prevent the disease. If they test negative, they should not think that they won’t get the disease and ignore safe lifestyle. People should follow the same advice if they test negative for the melanoma associated genes. Patients should disclose their results with doctors. If they are at risk for developing melanoma, they should make dermatologists aware so that the patient can take preventative measures.
Carbone, M., Yang, H., Pass, H. I., Krausz, T., Testa,
J. R., & Gaudino, G. (2013). BAP1 and cancer. Nature reviews. Cancer,
13(3), 153–159. doi:10.1038/nrc3459
CDKN2A. (n.d.). Retrieved from
https://www.snpedia.com/index.php/CDKN2A.
Dickens, B. M., Pei, N., & Taylor, K. M. (1996).
Legal and ethical issues in genetic testing and counseling for susceptibility
to breast, ovarian and colon cancer. CMAJ: Canadian Medical Association journal
= journal de l’Association medicale canadienne, 154(6), 813–818. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1487772/
Hayward, N. Genetics of melanoma predisposition.
Oncogene 22, 3053–3062 (2003) https://www.nature.com/articles/1206445#citeas
Melanoma – Genetics Home Reference – NIH. (2018,
August). Retrieved from https://ghr.nlm.nih.gov/condition/melanoma#statistics
Melanoma Survival Rates. (n.d.). Retrieved from
https://www.curemelanoma.org/about-melanoma/melanoma-staging/melanoma-survival-rates/
rs387906848. (n.d.). Retrieved from
https://www.snpedia.com/index.php/Rs387906848
Should I Get Genetic Testing For Melanoma? (n.d.).
Retrieved from
https://www.aad.org/diseases/skin-cancer/melanoma-genetic-testing.
In Star Wars Episode II Attack of the Clones, Obi-Wan Kenobi steps off his shuttle onto the planet Kamino in order to track an intergalactic killer. Instead of finding him, he stumbles upon a secret clone army being developed for the Republic, one clone exactly the same as the one before him. They are all being based on one man, Jango Fett, who happens to be the killer that Obi-Wan is tracking this whole time. He was picked because he is of an optimal body type and a skilled shooter; he was a perfect template for an intergalactic army.
Don’t start sweating because you aren’t a Star Wars junkie
and have no idea what I’m talking about, this really goes beyond the point
here. During the year of Attack of the Clone’s release (2002), I am not
sure that anyone actually thought that engineering an army of men who were
equally lethal, loyal, and dangerous was possible. Just the mere idea of being
able to look at a person’s genome was unrealistic enough; why even try to
modify it? Potential advancements in the field of genetic modification (1),
such as CRISPR, have turned questions of possibility into questions of ethics.
Should parents be allowed to genetically engineer their
offspring? If so, to what extent should this be allowed? If not, what are the
foreseeable dangers of furthering research on genetic engineering?
What Are You Even Talking About?
To get us started, we must look at what is exactly meant by
genetic engineering. Genetic engineering is defined as “a group of applied
techniques of genetics and biotechnology used to cut up and join together
genetic material and especially DNA from one or more species of organism and to
introduce the result into an organism in order to change one or more of its
characteristics.”(2) Lengthy definition, I know. Let me break it
down for you:
Genetic engineering appears to do one thing to achieve one
purpose. It changes or influences the genetic makeup of an organism in order
for that organism to exhibit one or multiple desired traits. In a sense, it is
like me baking a cake. In order for me to make a regular cake exhibit chocolate
taste, I would need to add some cocoa powder to make the cake show that
specific characteristic.
The focus of this article is not to outline all the new and
shiny technologies that can allow us to influence our genetics nor am I determining
the potential of genetic engineering. Instead, I hope to point to the direction
that modifying the genome can take us.
The Positives: Disease Therapy
The concept was born out of a need to create a cure for certain genetic diseases. CRISPR can be used to modify disease-causing variants in the genomes of embryos and to remove such variants for other generations as well.(3) Doctors could edit immune cells to better fight cancer or edit blood cells to cure sickle cell anemia. There are many diseases that don’t currently have a physical cure, so genetic therapy could prove to be an effective alternative to remedy these diseases. It is for this reason that genetic engineering seems wildly attractive, for it supplies a possible solution to a problem that has large urgency. It appears that millions of lives can be saved through this medical practice. If the medical community can remove a child’s ability to have cystic fibrosis in the future or cure a current victim of cystic fibrosis, why shouldn’t they be able to?
The Other Side
Like with every advancement in society, whether it be technological or, in this case, medical, there are several compelling arguments against the usage of genetic engineering.
1. Health Risks
How would pregnancies be affected as a result of using altered embryos? The medical community overall has very little conclusive evidence over the safety of mothers and even modified offspring. (4) Genetic engineering could result in many miscarriages and paternal deaths. Sure, this problem could be resolved with further development, but performing human clinical trials presently could prove costly.
2. The Class System
A perhaps off-putting characteristic of genetic modification is its cost. Editing the genome of an individual is likely to be costly, especially if many specific demands are desired. The only families that could afford such adjustments would be upper-class individuals. (1) Such families, in theory, could create model children with peak physical and intellectual traits. What results is an increasingly polarized class system. Society would have an upper-class dominated by offspring that genetically are better off for future success, and a middle-class and lower-class with unedited offspring that are simply disadvantaged compared to upper-class offspring. With very limited social class movement resulting, modifications could create classes of individuals defined by the quality of their genome. (1)
3. Discrimination
For a world that so publicly expresses their
dislike for racism and discrimination, genetic engineering in a sense
reinforces our biases. (4) Particularly in South Asian regions,
having lighter skin is a sign of high class and poise. (5) If people
in that area can choose traits that make their children have lighter skin, that
beauty trend would be further enforced. This goes beyond just appealing traits;
gender distribution is at stake as well. In 2015, it was reported that 21
countries had an abnormal distribution of males and females. (6) Many
of these cultures just have a preference for sons rather than daughters. That
being said, the combined technology of sonograms and genetic engineering could
allow people to know the sex of their child as well as decide it as well. Should
this technology become more generalized or more accessible, this could throw
the balance of gender off balance: a harmful abundance of men compared to women
or vice versa. Humanity would be disadvantaged as it pertains to reproduction,
for there simply wouldn’t be enough women to create life with.
Physical vs. Psychological, Present vs. Future
What’s interesting about the arguments against genetic
engineering is that most potential negative consequences occur far into the
future. The benefits of the system can be seen almost instantly. There is tech,
such as CRISPR, at the ready to spot genetic diseases. Saving the lives of many
presently seems to be the most important matter since it is the most present
issue. It is for that reason that it can perhaps be difficult to turn down the
continuation of research in this field. On the contrary, since the technology
currently isn’t widespread or advanced, it is easy to write off the dangers as
outlandish slippery slopes. The overarching negative consequences could be considered
too farfetched or unrealistic to be believable simply because they are futuristic.
We must recognize here that furthering the research has physical benefits but a lot more psychological and emotional detriments. In the future, the medical community could find possible cures to multiple currently incurable diseases. Genetic engineering, while the most straightforward route, is not the only solution to world disease. Furthermore, the mere possibility of intense class and trait discrimination looms large. Logically, genetic engineering has the potential to output the negative consequences mentioned above. While we can’t rule out the good that gene therapy could do, foresight can tell us that allowing genetic engineering to advance and apply itself past what’s necessary has extreme fallouts.
Look! Sources.
“What Are the Ethical Concerns of Genome Editing?” National
Human Genome Research Institute, 3 Aug. 2017
“Genetic Engineering.” Merriam-Webster
“Pro and Con: Should Gene Editing Be Performed on Human
Embryos?” National Geographic, 26 Nov. 2018.
“What Is Human Gene Editing?” Center for Genetics
and Society
Pe, Roger. “Yes, Asia Is Obsessed with White Skin.” Inquirer
Business, 1 Oct. 2016
Brink, Susan. “Selecting Boys Over Girls Is A Trend In
More And More Countries.” NPR, 26 Aug. 2015
With the development of medicine and DNA technology, we have known for some time that diseases like breast cancer and ovarian cancer is tied to genetics. Similarly, we have recently found more evidence that prostate cancer in men is also linked to genetics which, on a lighter note, can lead us to even more early identification of this cancer in men around the world.
What?
According to SNPedia, a risk model for prostate cancers is based on two major predictors. The first is family history and inherited genetic mutations. The traits and code passed to you from your parents; or a genetic mutation, which is a permanent alteration in the DNA sequence for a gene. The second is 5 SNPs. SNPs are the most common form of genetic variation in individuals, each one represents a difference in a single DNA nucleotide.
Research has shown a connection of some type between individual types of prostate cancers and inherited mutations in BRCA1, BRCA2, ATM and CHEK2. BRCA 1 and 2 are both genes that produce tumor suppressor proteins. ATM is also a gene that makes proteins that when mutated increases the risk of cancers. The CHEK2 gene provides instructions for making a protein called checkpoint kinase 2. This protein acts as a tumor suppressor
The 5 SNPs chosen to represent five regions of chromosomes 17q12, 17q24.3 and 8q24 (three regions) are rs4430796, from ch 17q12, rs1859962, from ch 17q24.3, rs16901979, from ch 8q24 (region 2), rs6983267, from 8q24 (region 3), and rs1447295, from 8q24 (region 1).
These are the gene sequences and mutations tested to help address aggressive types of prostate cancer in men.
Who?
There are, according to the Urology Care Foundation, two groups of men that should actively consider genetic testing for prostate cancer.
The first group is men with localized prostate cancer who also have a family history of breast, colon, ovarian, pancreatic or prostate cancer. Localized means that the cancer has not spread outside the prostate. The reason why men with this type of cancer should consider being tested is that it can identify mutations in genes that could be harmful or be passed to offspring, rather than assess the risk of developing prostate cancer.
The second group of men who may want to think about genetic screening are those with metastatic prostate cancer. Metastatic prostate cancer is a type of cancer that has spread beyond the prostate into other areas of the body. A recent study found that nearly 12 percent of men with metastatic prostate cancer will have a genetic mutation present. This discovery can help lead to various treatment plans for patients, which brings me to my next point.
Why?
Getting the news that you have a genetic mutation linked to prostate cancer benefits your whole family. They too may now consider testing to see if they also inherited the gene. Moreover, men with a family history of a genetic mutation should start getting screened for prostate cancer earlier than men who do not. BRCA1 and BRCA 2, two of the genes in question have an autosomal dominant pattern of inheritance while ATM and CHEK2 are passed in an autosomal recessive manner.
On the contrary, there is speculation about the drawbacks of using genetic testing haphazardly with men. While screening helps many patients and their families, there is concern that we could begin to overuse genetic testing prematurely in men for a type of cancer that more men die with than die of, according to AARP.
The main reason to get genetic testing is if you have been diagnosed with a form of prostate cancer or it runs in your family so you can educate your family about the importance of early detection. The misconception that all men need to get screened for early detection can lead to overuse of screening as well as premature testing which is costly, time-consuming, and stigmatized. There is also, however, the benefit screening provides to men who do not have prostate cancer of alerting them to mutations that put them at a higher risk, etc.
Another caution in genetic testing is the possibility of false-negative and false-positive test results. According to a Harvard Medical School study, the test failed to predict 95% of cancer in the sample of men, as well as 2.2% of men without cancer in the study were lead to worry about an increased risk of cancer. This worry is another caution of screening for men.
There are also ethical questions as well as psychosocial risks which include guilt, anxiety, impaired self-esteem, social stigma, and discrimination when it comes to employment or insurance.
You should ask yourself all these questions if you are considering genetic testing for prostate cancer.
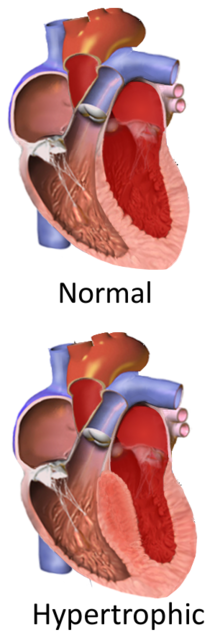
Familial Hypertrophic Cardiomyopathy is a rare heart condition where the heart muscle thickens, blocking blood flow to the body. The muscle thickening typically occurs in an area of the heart known as the interventricular spectrum, which separates the two lower chambers of the heart. In some patients this muscle thickening can lead to abnormally sounding heart beats, which can obviously be detected. In other cases, however, there may be no visible or audible symptoms, just slowed blood flow, which can be very serious. Regardless, the thickening of the muscles in the heart obstructs the flow of blood into and out of the heart, which can be fatal. The prognosis for individuals affected with FHC is relatively benign- those affected may live for years without any symptoms or issues. A study by Thoraxcentre in The Netherlands has shown that, “HCM has a relatively benign prognosis (1% cardiac annual mortality) that is 2-4 times less than previously thought.” According to the US National Library of Medicine, Familial hypertrophic cardiomyopathy affects an estimated 1 in 500 people worldwide. It is the most common genetic heart disease in the United States.” It is a gene that is autosomal dominant, so both parents must be at least carriers for the offspring to have a chance of having Familial Hypertrophic Cardiomyopathy. Autosomal means that the FHC gene is located on a non-sex chromosome, so both male and female offspring have an equal likelihood of receiving a copy. Dominant means exactly what is seems- it only takes one copy of the gene mutation to cause the disease. Therefore, when an offspring receives genes from its parents, it only takes one mutation in the MYH7 gene, or any other gene linked to FHC, to cause Familial Hypertrophic Cardiomyopathy. There are close to ten genes with variations that could leave the patient affected by FHC. The most prevalent mutation is in the MYH7 gene, which is associated with about 35% of FHC cases.
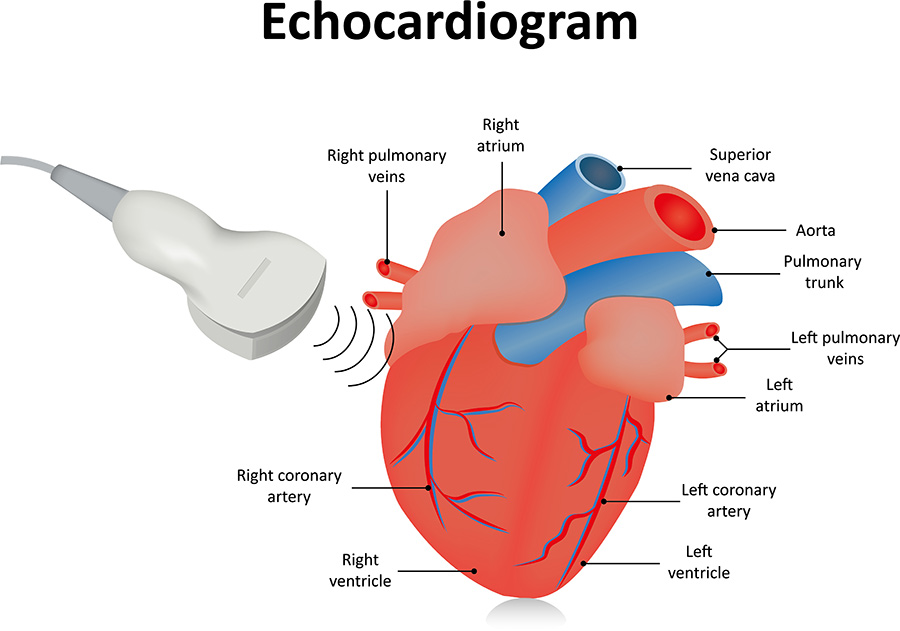
In order to identify Familial Hypertrophic Cardiomyopathy, it is imperative to get tested. Testing can be especially important in athletes and highly active people, because they are the ones that are physically exerting themselves the most, and their heart rates are, on average, higher. When an athlete is playing a sport, such as basketball, their heart rate is high, and their heart is having to work harder in order to get oxygen-rich blood to the body. If muscle is thickened, it is more difficult for the heart to distribute blood to the body. At higher heart rates, the heart can become overworked and blood may cease flowing and clot, which can be fatal. The most effective way to test for FHC is through an Echocardiogram, which is an imaging test where a doctor can see if the heart muscle is abnormally thick. Genetic Testing is not the most effective way to test, as results may not provide any definitive answer. One reason for this, according to the Mayo Clinic, is that, “Only about 50 percent of families with HCM have a currently detectable mutation, and some insurance companies may not cover genetic testing.” I would recommend some form of monitor testing, something that allows doctors to see if the heart muscles are enlarged or not. It can cost up to two thousand dollars for an echocardiogram, and no options that test the heart are cheap. Without insurance, you may still need to pay the entire cost by yourself. With insurance that does in fact cover an Echocardiogram, there will still be a co-pay of up to one thousand dollars. Even genetic testing would be expensive to test for all the gene mutations associated with FHC.
Before getting tested for Familial Hypertrophic Cardiomyopathy, it is important to know as much as possible about possible issues or limitations with the test. For example, there are about ten genes with variations, and some only account for a small increase in risk. Even with that mutation, it is still very possible that the patient will not have FHC. Also, there could be an undetected variation that the patient has that is not known to cause FHC, but it could because it just has not been associated to it yet.
There are many other possible repercussions to being tested for potential FHC. One is the possibility of your genetic information being sold to outside companies. Your genetic privacy is very important, and it could be a big problem if your information is sold. The company 23andMe is an online platform where you mail in a sample and get your results within a couple of weeks. According to the website, “Everyone deserves a secure, private place to explore and understand their genetics. At 23andMe, we put you in control of deciding what information you want to learn and what information you want to share.” There are also some potential downsides of being genetically tested for Familial Hypertrophic Cardiomyopathy, mainly because only about half of the people who have FHC in their genetic makeup have a detectable gene that will show they have it. In addition, it is very difficult to live knowing you have Familial Hypertrophic Cardiomyopathy, as you must exercise extreme caution whenever doing any physical activity. Treatment can help, and knowing about the disease could be lifesaving, especially for college athletes. College athletes, in particular, should know if they have FHC, because it could be lifesaving. It is important for all athletes to be tested, but I believe it should be required for collegiate athletes in the United States.
When being tested for Familial Hypertrophic Cardiomyopathy, it is important to be educated and ask the right questions to the experts. It depends on the gene in question, but since FHC is autosomal dominant, if a parent has tested positive, then there is a good chance a child will also test positive, about fifty percent. According to the National Library of Medicine, “This condition is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder.” It also states that, “In most cases, an affected person has one parent with the condition.” If they test positive, they should consult with the doctor and ask about possible treatments to help with the condition and about what they should do regarding physical activity. If they test negative, they should still be careful about physical activity or maybe even get a second test if possible, because of how much of a toss-up genetic testing is for FHC. I would tell my doctor anything I know, because they probably know more than I do and could help me out in my lifestyle changes. If they test positive, I would recommend screenings like the echocardiogram, because it can be far more definitive than the genetic testing can be, and the doctor can tell you the level of severity at the given time. A positive test should result in significant changes to the affected person’s life. They should be very careful when doing any physical activity, and they should limit their exertion.
In conclusion, Familial Hypertrophic Cardiomyopathy is a very serious heart condition that is genetic. People who have it in their genetic history should definitely get tested. I would recommend first getting an echocardiogram, to test the heart valves and muscles associated with FHC. If they are in fact swollen or enlarged, then I would recommend the genetic testing for FHC. Even though the results are inconclusive, you may be able to conclude more after echocardiogram results have come back. For example, if you know that heart muscles have thickened, you could pair that information with your genetic testing in order to develop the most conclusive results possible. It is very important to detect it, as it could be lifesaving to know that you have it, because treatments and lifestyle changes can have big effects. Before being tested for FHC, it is imperative to know as much as you can about the tests and ask the right questions.