
Community-Based Interventions Implemented in Combination to Improve Vaccination Rates
Table 1. Summary of Recent Interventions
| Author & Year | Intervention Setting, Description, and Comparison Group(s) | Study Population Description and Sample Size | Effect Measure (Variables) | Results including Test Statistics and Significance | Follow-up Time |
| Aragones, Bruno, Ehrenberg, Tonda-Salcedo, & Gany, 2015 | Mexican-American parents attending the Health Window Program at the Mexican Consulate in New York City were recruited to participate in a study utilizing parental education and text message reminders to increase HPV vaccination completion rates among Mexican American children.
All study participants were given a one on one educational session with a trained health worker and then were either assigned to receive no text messages and or to receive text reminders (in Spanish) regarding their child’s vaccination status and eligibility. Messages were sent weekly until completion of 1st dose, and one month before due dates of the second and third doses. Messages were sent weekly until dose completion was confirmed via telephone. |
Eligible parents were selected, meeting the following criteria: Mexican-American parent, 18 years of age or older, speaking Spanish as a primary language, in possession of a text-capable cell phone, and who is the primary caregiver of at least one child between the ages of 9-17 who has not received the HPV vaccine; n=69. (All received brief one on one educational session, 24 were assigned to control group, & 45 were assigned to intervention) | Outcome measures included completion of full HPV vaccination course (3 doses) for a parent’s youngest eligible child. | Parents receiving text message reminders were 15.5 times more likely to complete the HPV vaccination course than those in the group not receiving text messages (p<0.001). Variables shown to have no association with the outcome include gender of parent or child, parent age, English proficiency, or prior knowledge of the vaccine. | Phone call follow-ups (in Spanish) were conducted with parents to determine child vaccination status at:
1) 6 weeks after failure to receive 1st dose or 2) 4 months after completion of second dose to assess 3rd dose completion |
| Yoo, Humiston, Szilagyi, Schaffer, Long, & Kolasa, 2015 | Elementary school children in Monroe County, New York during the fall seasons of 2009 and 2010 were enrolled in a community-based randomized controlled trial examining the effectiveness, cost, and cost-effectiveness of school-located vaccination against influenza (SLV).
The study randomly assigned 21 elementary schools as the intervention schools or intervention group for 2009 and 2010. Ten and eleven elementary schools were randomly assigned as the control group for 2009 and 2010 respectively. |
A total of 31 and 32 elementary schools in the Monroe County area were included in the 2009 and 2010 studies respectively. The intervention group included 21 schools and the control group included 10 and 11 in 2009 and 2010 respectively. There were 9027 students enrolled in the intervention schools in 2009 and 9145 students in 2010. The control group had 4534 students enrolled in the 10 schools in 2009 and 4796 students enrolled in the 11 schools in 2010. | “Cost effectiveness analysis (CEA)” – Measured as the cost effectiveness ratio. This was calculated by dividing the incremental cost (i.e. the difference in cost of intervention schools minus the cost of vaccination in control schools) by the incremental effectiveness (the number of additionally vaccinated students in intervention schools vs control schools)
“Effectiveness”- measured by overall influenza vaccination rate. Defined as “the difference between the proportion of students who received ≥1 seasonal influenza vaccine anywhere among students enrolled in the intervention vs the control schools.” “Costs” – measured in U.S. dollars this was a total sum of the program costs broken down into school costs, project coordination costs, and vendor costs |
Overall, rates of influenza vaccination of children in the intervention group were 40.7% and 40.4% in 2009 and 2010 respectively, while rates of influenza vaccination of the children in the control group were 29.8% and 28.4% in 2009 and 2010 respectively. This study found that children in schools with SLV programs are 1.5 times more likely to receive at least one seasonal influenza vaccine (p-value<0.0001). When averted costs were not taken into account, it was found that SLV vaccination programs are more costly than individual private practice administration. When averted costs were taken into account, the cost for SLV programs was comparable or lower than primary care practice. | No follow up. |
| Willis et al., 2016 | Community Health Improvement for Milwaukee Children (CHIMC) launched educational, social marketing, and planned behavior interventions in an effort to reduce vaccination disparities among children age 19-35 months in lower socioeconomic families, using a community-based participatory research (CBPR) approach. (Vaccinations in question: DTaP/3HPV/1MMR/3HepB/3Hib/1VZV antigen series). Participants were recruited from target communities and completed a survey consisting of demographics, immunization beliefs, and psychosocial factors. An educational presentation was given to participants and pre- & post-knowledge surveys were obtained along with immunization rates. Initial surveys were used to create a social marketing campaign, disseminated it throughout the communities, and conducted surveys to test the reach of the campaign. Planned behavior change intervention worked to identify barriers to parents’ keeping children up to date on vaccinations and demonstrated ways of navigating the healthcare system. | 565 parents/caregivers and 1,533 children were enrolled and surveyed by CHIMC. (89.4% female, 91.4% African American, 63.5% unemployed, 70.5% single-headed households, 78.3% mother/child relationship with child participant). Of the households, mothers made the immunization decisions in 82.3% of them. | Education interventions measured pre and post intervention attitudes and knowledge relating to child vaccination and compared changes in immunization status. It also examined immunization status between children’s age group and sought to identify factors influencing parents’ perception of vaccination.
The social marketing campaign measured the amount of people who had seen the CHIMC’s messages and to what degree they were able to recall it, as well as their attitudes towards vaccinations. The planned behavior change intervention identified the most common perceived barriers to child vaccinations. |
Baseline data was found to be different from that in Healthy People 2020. Educational interventions yielded a significant increase in both vaccination knowledge and increased immunization status from baseline (p<0.05). Of the 408 participants surveyed about the social marketing campaign 51% recalled a message about children’s health but only 2% were able to recall the CHIMC’s message. The planned behavior change intervention identified the most commonly noted barrier to child vaccinations were hospital personnel (rhetoric, attitudes) and limited resources (time, transportation, insurance issues). | The follow-up time for recall and immunization status of study participants occurred over 8 years. The CHIMC is ongoing and will continue to implement community-based approaches to develop interactive information dissemination about child vaccinations. Resources will be compiled at www.chimcke.org. |
Community Guide Update and Rationale for Intervention
Based on the selected strategies explored within these articles, the implementation of community based interventions, implemented in combination, to increase rates of vaccination are still strongly recommended which is in agreance with the 2014 Task Force finding. Recent intervention programs such as text message reminders to increase HPV vaccine compliance, school located vaccine programs, and educational programs have shown statistically significant improvement in vaccination rates, especially in communities of lower socioeconomic standing where disparities are more pronounced.
Intervention strategies implemented at the community level have shown to be effective at increasing vaccination rates. Community-based combinations of interventions performed after the 2014 Task Force recommendations were published have proven to yield significant increases in vaccination compliance rates across various age groups and demographic groups.
In their community based intervention involving an educational session on HPV vaccinations, followed by text message reminders, Aragones et al. found that parents receiving text message reminders were 15.5 times more likely to complete the HPV vaccination course than those in the group not receiving text messages. This study involved 69 Mexican American families with children under age 18 who had not received the HPV vaccine. After a brief one-on-one educational session, parents were assigned to groups that did and did not receive text message reminders about when their child was due for their next HPV vaccine booster. They measured completion of full HPV vaccination course (3 doses) for a parent’s youngest eligible child and found no other significant association (gender, age, English proficiency) between increased vaccination rates, other than having received text message reminders.
Willis et al. employed textbook example of the Task Force’s recommendation; a community level multi-component approach, incorporating voluntary educational sessions, a social marketing campaign, and a planned behavior change intervention. While the planned behavior interventions and the educational sessions were more effective than the social marketing campaign, all of these interventions produced significant results. This intervention targeted lower socioeconomic communities and was composed of mainly females and African Americans, including 565 adults and 1,533 children. The Community Health Improvement for Milwaukee Children’s educational campaigns yielded a significant increase in both vaccination knowledge and increased immunization status from baseline (p<0.05) (Willis et al.) About 208 out of 408 people within the community were reached by the social marketing campaign and the planned behavior change intervention identified the most commonly noted barrier to child vaccinations included hospital personnel and limited resources such as time and money, providing the city of Milwaukee with valuable information on how to best provide community-based vaccination programs.
Finally, Yoo et al. found results consistent with the recommendations outlined by the Task Force as well, with their study on the effectiveness of school-located vaccination against influenza. They found that vaccination rates among children in the intervention group were about 11-12% higher than children in the control group. Children in schools with SLV programs are 1.5 times more likely to receive at least one seasonal influenza vaccine (p-value<0.0001) (Yoo et al.) This study also found that SLV programs was comparable or lower than primary care practice when averted costs were taken into account. The SLV program intervention study went on for two years and included a total of 31 and 32 two elementary schools in Monroe county in New York, either year. Slightly more 9000 students were enrolled at either school and roughly half of the children were placed in the intervention group, with the other half in the control group.
Aragones et al. targeted parents of Mexican-American children and was greatly successful in increasing the rates of vaccination within the target population. Willis et al. improved attitudes concerning childhood vaccination among communities of low-socioeconomic standing. Yoo et al. found that children with access to school located vaccine clinics were much more likely to receive recommended vaccinations. All three of these studies exemplify the potential for community based combinations of interventions to increase vaccination among targeted communities.
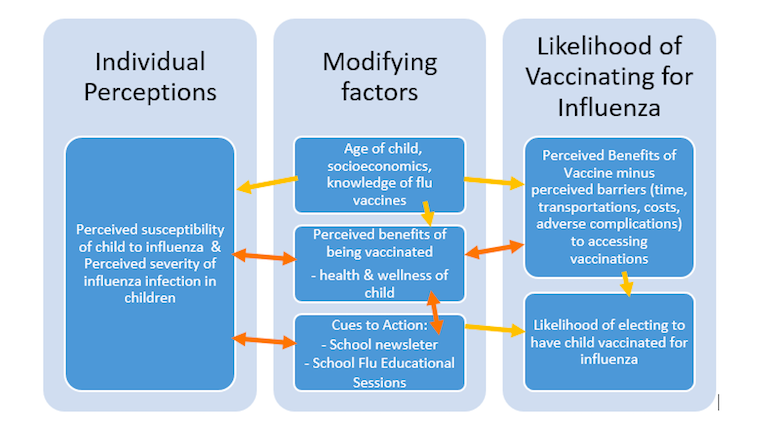
Theoretical Framework/Model
The Health Belief Model and the Community Based Interventions Implemented in Combination to Increase Appropriate Vaccination
The health belief model (HBM) is an explanatory model that, at the time of its conception, was primarily used as a technique for determining why many people do not participate in disease prevention programs (Rimer & Glanz, 2005). The HBM approaches the desired behavior on an individual level, focusing on an individual’s perception of health condition, the degree to which they feel the condition is a threat to them, and the marginal benefit of taking action once the cost of potential barriers to action are overcome. These factors determine the likelihood of an individual making a behavior change. This was model excellently demonstrated by Willis et al. in the Community Health Improvement for Milwaukee’s Children Program, an ongoing community-based approach to identifying misinformation and barriers to early, childhood vaccination, and subsequently disseminating educational information and effective access to resources. If we care able to effectively educate people on vaccinations we can correct any misinformation, quell some irrational fears, and provide information on effective methods of vaccination. Education at the community level affords the opportunity to target specific groups who may be disproportionately affected by a preventable disease and who would benefit more from certain vaccinations. Identifying perceived barriers to vaccination guides our objectives towards reducing those barriers and/or revealing resources already available to people.
Constructs
- Perceived susceptibility: This describes what a person perceives as their chances of being affected by a particular condition. As described by Aragones et al., Latinos in the U.S. are disproportionately affected by HPV and are therefore more susceptible to associated complications. This is directly linked to how severe a threat a person feels the condition presents to them, which affects the likelihood of their pursuing vaccination. Part of our intervention, through educational seminars, is to improve the accuracy of parents’ perception of their child’s susceptibility to preventable diseases, for which vaccinations exist, such as influenza.
- Perceived severity: This goes hand in hand with perceived susceptibility. Although a person may be highly susceptible to a condition, they may be more likely to act and receive vaccination if the perceived severity of the disease is high. Alternatively, if an individual feels that a disease would not be severe, they may not feel threatened by it. In turn, they may then feel that the receiving a vaccination may not be worth the hassle. Once again, the educational seminars through the elementary schools will provide parents with the information needed to assess the severity of a disease for which a vaccine exists, like influenza.
- Perceived benefits: These are the perceptions an individual has relating to how effective an action would be at reducing the risk of a disease. Our recommended intervention incorporates educating parents on how and when to take action, as well as the expected positive results of such actions
- Perceived barriers: These are the perceptions an individual has relating to the tangible and intangible costs of taking action. Willis et al. excellently identified many common barriers parents faced when attempting to have their children vaccinated, and correcting common misinformation and offering reassurance to uncertain parents. Our recommended intervention incorporates this construct at the community level through Athens-Clarke County elementary schools, emphasizing the importance of increasing access to preventative health care by offering school located vaccination clinics.
- Cue to Action: These are factors that may be likely to elicit an action. Commonly these are exposed to factors that prompt action. Willis et al. studied the effects of a social marketing campaign and it’s effects on people’s perceptions towards childhood vaccinations. Aside from media, other factors could be education or reminders, such as those utilized by Aragones et al. where using text message reminders led to a significant increase in HPV vaccination series completion. Our program will utilize various outlets to reach elementary school parents on the importance of the annual influenza vaccine for elementary aged children.
- Self-efficacy: Perhaps the most critical construct within the HBM, a person’s confidence in their own ability to initiate an action. In terms of vaccination, people need to be aware of their options, and confident in their understanding of the associated disease. This will in turn determine how confident they feel about initiating a behavior change, and pursuing vaccination options. Community-based outreach programs implement measures that empower people to make confident decisions about their health. For our program, we will define and measure the concept of self-efficacy by directly evaluating the participating parents’ perceived knowledge and attitude towards influenza vaccination for their children.
Conceptual Model Diagram
Target Population and Program Settings
The target population for community based interventions implemented in combination to increase vaccination are those populations that presently have low vaccination rates. For our specific program utilizing this task force suggested intervention, the target populations consist of elementary school aged children that have not received the annual influenza vaccine in the past 3 years and those children’s parents in the Athens-Clarke County school district. Athens-Clarke County consists of discrete populations of minority and low-socioeconomic citizens which are at greater risk for health disparities such as low vaccination rates and outbreaks of vaccine preventable diseases. Because of these varying populations within Athens-Clarke County, our program will initially target families that do not regularly seek out the annual influenza vaccine for their children. This will be accomplished through a screening survey at the start of the school year in August.
It is critical that children under the age of 12 receive childhood recommended immunizations so as to prevent communicable diseases that are vaccine preventable (CDC 2016). It is also critical that a certain percentage of school aged children receive seasonal influenza vaccines so as to help prevent potential influenza outbreaks in school. While pediatricians are often the primary providers for vaccination of school aged children, it has been found that children very infrequently seek out primary care for non-acute or preventative care (Rand, 2007). Our program will specifically address increasing seasonal influenza vaccination among school aged children in Athens-Clarke county.
“2016 Recommended Immunizations for Children from Birth Through 6 Years Old,” CDC, 2016.
Rand CM, Shone LP, Albertin C, et al. National health care visit patterns of adolescents: implications for delivery of new adolescent vaccines. Arch Pediatr Adolesc Med 161:252-259. 2007.
Logic Model, Intervention Hypotheses, and Intervention Strategies
Table 2. Increasing Appropriate Influenza Vaccination with Community-Based Interventions as Related to the Health Belief Model (HBM) of Behavioral Change.
| Intervention Method | Alignment with Theory | Intervention Strategy | |||
|
The HBM construct of likelihood for action is perfectly demonstrated by this intervention method. Reducing barriers for children and their families to receive the seasonal flu vaccine through both community education and school located vaccination programs is in line with this construct, as the model describes that individuals are much less likely to change a behavior if the perceived barriers of accessing the intervention are greater than the perceived benefits of that access. Therefore, when implementing a successful combination and community based influenza vaccination improvement program, it is essential that the community members view accessing influenza vaccination as a relatively simple and painless process. | Reducing barriers to the influenza vaccination can be achieved through several strategies. Children (and parents of children) will be provided with more opportunities to access influenza vaccination through school-based vaccination programs. Children enrolled in Athens-Clarke County schools and their family members will have the opportunity to receive a seasonal influenza vaccine in a convenient and affordable manner through this program. | |||
|
|
|
|||
|
|
|
|||
Table 3. Program Logic Model
| Inputs/Resources | Activities | Outputs | Short-term Outcomes | Intermediate Outcomes | Long-term Outcomes |
|
Funding for educational meetings and materials targeted at parents regarding seasonal influenza vaccination. Personnel, including educators, community leaders, social marketing teams, and trained medical professionals (nurses, M.D.’s, local health department, etc). Partnership with local organizations such as clinics, schools, churches, and organizations where parents of school aged children may be effectively reached and where educational information can be placed. Announcements regarding the seminars should be disseminated through school newsletters and emails. Partnership with board of education so that school located vaccination programs can receive adequate support and funding. Space where lectures/educational session can be held. |
Dissemination of educational information regarding seasonal influenza and the importance of receiving vaccination, particularly among school aged children. This will be achieved through pamphlets and educational sessions.
Educational sessions will take place at elementary schools 4 times per month during August, September, and October with local Athens-Clarke County pediatricians and other health professionals. These 12 educational events will take place the three months before the start of the school located vaccine clinics so that parents have adequate time to prepare and register. The school located vaccine clinics will occur through November, December, and January. Program will also reinforce the roles of medical professionals in their responsibility to educate parents and promote available vaccination resources. Specific target community, school aged children, is one with low vaccination rates for influenza (59.3% in 2014/2015 school year) (CDC, 2016). Elementary aged children are also at increased risk of developing complications related to influenza (Longini & Halloran, 2005). Therefore activities are specifically aimed at increasing the rate of influenza immunization among school aged children. |
Outputs will include stocks of the annual vaccines for each of the 14 Athens-Clarke County elementary schools. Stocks of the vaccine will include enough so that vaccination can be offered to children’s family members as well during the school located clinics hosted in November, December, and January. Consent forms, letters, and educational pamphlets will be drafted and provided to all 14 elementary schools. Training materials for health professionals administering vaccines and any participating school staff will be created and distributed. | Reduce barriers for children and their families to receive the seasonal influenza vaccine through the school located vaccine clinics.
Improve parent knowledge about immunization, specifically influenza vaccination through the educational seminars. Improve parent attitude regarding immunization, specifically influenza immunization through the educational seminars.
|
Increase rates of influenza vaccination in Athens-Clarke County school children during the 2017 school year. Continued support for school located influenza vaccination programs in the Athens-Clarke County areas and potentially surrounding counties. |
Potential application of the program for other vaccine preventable diseases. Decreased annual rates of influenza symptoms in school aged children in Athens-Clarke County. |
“Flu Vaccination Coverage* by Race/Ethnicity, Children 6 months–17 years, United States,† 2014–15 Season.” CDC. 2016. http://www.cdc.gov/flu/fluvaxview/coverage-1415estimates.htm#data
Longini, I. M., Jr., & Halloran, M. E. (2005). Strategy for distribution of influenza vaccine to high-risk groups and children. Am J Epidemiol, 161(4), 303-306. doi:10.1093/aje/kwi053
Intervention Hypothesis
Dissemination of educational materials and educational seminars hosted for parents during the months of August, September, and October will increase parent knowledge and improve parent attitude concerning influenza vaccination in children in Athens-Clarke County. The seminars will be hosted and conducted by various health officials and will be critical in providing accurate, concrete information for parents in Athens-Clarke County. They will also be outlets for open and honest discussion regarding influenza vaccination as well as other recommended vaccinations for children.
The school located vaccination clinics hosted during November, December, and January will reduce barriers for Athens-Clarke county children and their families to receive an annual influenza vaccine. These clinics will hopefully increase the rate of influenza vaccination among Athens-Clarke county elementary school children.
Causal Hypothesis
Based on the application of the Health Belief Model construct and our projected outcomes, the reduction of barriers for children and their families to receive the seasonal influenza vaccine through the school located vaccine clinics will lead to increased rates of influenza vaccination in Athens-Clarke County school children during the 2017 school year. This direct reduction of barriers and enhanced access to the influenza vaccine may prompt the potential application of the program for other vaccine preventable diseases as well as contribute to continued support of the established school located influenza clinics in the Athens-Clarke County elementary schools. Improvement if parent knowledge and attitudes regarding immunization, specifically influenza vaccination through the educational seminars will also contribute to increased rates of influenza vaccination in Athens-Clarke County school children as well as contribute to continued support for school located influenza vaccination programs in the Athens-Clarke County areas and potentially surrounding counties. Increasing the knowledge base and improving the attitudes of parents will, in the long run, increase the rate of influenza vaccination among Athens-Clarke County school children and therefore decrease annual rates of influenza symptoms in Athens-Clarke County school children.
SMART Outcome Objectives
Goal 1: Reduce barriers for children and their families to receive the seasonal influenza vaccine through the school located vaccine clinics.
Objective 1: Screening of Athens-Clarke County elementary school parents will establish the target population and baseline for our program. Parents that have not vaccinated their children in 3 or more years will complete surveys in August 2017 evaluating their perceived barriers to accessing the influenza vaccine for their child or children. The same survey will be provided at the end of January 2018 (the last month of the school located clinics) as well as at the start of the next school year, August 2018. We would like to see at least a 75% increase from our baseline in number of parents reporting easy, simple outlets to vaccinating their elementary school children in January 2018 and at least a 50% increase from our baseline in August 2018.
Goal 2: Improve parent knowledge about immunization, particularly influenza vaccination through the educational seminars.
Objective 1: In the Athens-Clarke County community, parents should have outlets for various educational materials. This valuable information will be provided through the educational sessions hosted by the elementary school and led by Athens-Clarke County health officials. The same screening survey described in objective 1 will be utilized to evaluate the baseline knowledge of participating parents (those who have not vaccinated their child or children for influenza in the past 3 years). Using the same survey, we would like to see at least a 70% increase in reported understanding and competency of the influenza vaccine by participating parents in January 2018 and at least a 40% increase in August 2018.
Goal 3: Improve parent attitude regarding immunization, specifically influenza immunization through the educational seminars.
Objective 1: In the Athens-Clarke County community, parents should feel comfortable discussing concerns about immunizing themselves or their children with accessible and affordable health professionals. There should also be attempts to reach out to those that feel hesitant about vaccination. Discussions should always be open and non-judgmental of people’s backgrounds and beliefs. Any questions and concerns will be addressed at the educational sessions provided throughout the fall semester by an accredited medical professional. The same screening survey described in objective 1 will be utilized to evaluate the baseline attitude of participating parents (those who have not vaccinated their child or children for influenza in the past 3 years). Using the same survey, we would like to see at least an 80% increase in reported positive attitude towards the influenza vaccine by participating parents in January 2018 and at least a 50% increase in August 2018.
Table 4: Evaluation Design and Measures
| Stakeholder | Role in Intervention | Evaluation Questions from Stakeholders | Effect on Stakeholder of a Successful Program | Effect on Stakeholder of an Unsuccessful Program |
| Pediatricians, school nurses, and other participating health care providers (including Athens-Clarke County local health department) | These health care providers will carry a large role in effectively implementing the school-located vaccination programs as well as be critical for effective communication with parents regarding the importance of seasonal influenza vaccination for school aged children | Specific questions may include but are not limited to:
– Will this program be “worth their time”? – How many health care providers will be participating? – Will there be training for parent vaccination education? – Will physicians, nurses, or local public health officials be performing the vaccinations? – Will signed waivers of consent and proper parental approval be provided? – How will non school personnel be compensated for their time? |
Increased confidence in the school based programs. Decreased rates of influenza symptoms among children in Athens-Clarke county. Fewer uninsured children with unpaid medical bills. Decreased demand for unnecessary antibiotics from these health care professionals. | Feelings of having wasted time and energy were a waste leading to reservations about participating in future programs. |
| Athens-Clarke County school officials and staff | The officials and staff employed by the 14 elementary schools in the Athens-Clarke County school district will be critical in organization and execution of the school located influenza vaccination programs. Teachers and other school administrators will need to be involved in coordinating schedules and classes around the program days. | Specific questions may include but are not limited to:
– How will the school program affect classroom time? – Will teachers or other faculty be expected to chaperone during program days? – What options will be available for children not participating in the vaccine days? – Will school faculty be expected to contribute to parent conferences/ educational forums regarding childhood vaccination? Or will these sessions not include school staff? – Who will be responsible should a child have an adverse vaccine reaction? |
Fewer children missing school due to illness from the influenza virus. Increased confidence in the program. Increased sense of value in participating in the program. Fewer outbreaks of influenza within schools. | Feeling of having wasted classroom time due to dedicated program days. Unwillingness to participate in future programs. Protestations against participating in future programs.
Feeling of having wasted money and resources. |
| Parents with children in Athens-Clarke County schools | Parents will be at the forefront of the program for they will be responsible for participating in the community based education portion and applying this knowledge, by hopefully registering their children for the school vaccination programs. Without the cooperation and support of Athens-Clarke County parents, the program will undeniably be thwarted. Parents will be responsible for providing informed consent and allowing their children to participate in the vaccination program. It will also be important for parents to take roles in organizing the community education events, as other parents are most likely to take advice and heed the actions from their fellow community parents. | Specific questions may include, but are not limited to:
– Who will be vaccinating my child? Is it safe? What if something goes wrong? – Why are we choosing to focus on influenza and not other vaccines? – What happens if my child receives a vaccine and has a bad reaction? – Can my child still catch “the flu” after being immunized? – How will parents be expected to contribute to educational events and materials? – Will open discussions be provided for parents to voice their personal opinions on vaccination? – When will the program take place? – Can other family members take part in the program and receive vaccinations? – Are children currently suspended from school eligible to participate? – I’m a nurse, can I volunteer/ vaccinate my own child? |
Fewer children contracting the flu during the next flu season.
Parents actively seek out immunization for influenza in the future. Increased confidence in the value of this program and in the importance of flu vaccination. |
Lack of protections against the seasonal strain leading to sick children despite vaccination.
Feeling of having wasted time. Regret for having vaccinated children with no benefit. Parents doubting the effectiveness of vaccination programs and withdrawing their support from participating in future endeavors. Decreased likelihood of actively seeking out vaccinations on own in future. |
| Children in Athens-Clarke County schools | The most obvious stakeholders have the least control over this program. Children in Athens-Clarke county should be properly vaccinated against preventable diseases, like influenza, so that they can remain as healthy as possible. School aged children are the stakeholders who will most directly be impacted by this program, for they are the target population for increasing the rate of influenza vaccination. | Specific questions may include, but are not limited to:
– What is a vaccination? – Will it hurt? – How do vaccines keep people healthy? – Why do I have to do it? – How come we are getting shots at school? |
Increased tolerance by children to the idea of receiving vaccinations, even with the fear of the quick, temporary pain. Fewer children missing school due to the influenza virus, therefore performing better academically/extracurricularly.
Fewer school influenza outbreaks. Increased feeling of resentment by children for having to receive shots at school, despite success. |
An unsuccessful program could result in Athens-Clarke County children developing the same level of influenza symptoms as they would without increased rates of vaccination.
Increased feeling of resentment by children for having to receive shots at school. |
| Board of Education Athens-Clarke County School District | The Athens-Clarke County Board of Education is the stakeholder with the power of the purse. As the official governing body of the school district, the board members will be heavily involved in the implementation and funding for the community based education implemented in combination with school located vaccination in Athens-Clarke County. They will also be capable of determining the efficacy and validity of the program as well as in direct control of potential further expansion of the program. | Specific questions may include, but are not limited to:
– What is the timeline for the school located program? – When will educational programs and materials be implemented? – How much funding is required? – How many schools will be involved? – How will this affect a typical school day? – What are the risks versus the rewards? |
A successful program could result in the board expanding funding and potentially opening the program to include middle schools and high schools. It would provide the board with a new program to invest in and to advertise as a success. | An unsuccessful program could result in the board completely withdrawing support and funding for any future school located vaccination programs or vaccine education directed at parents. |
Evaluation Design: Quasi-Experimental Study – The Non Equivalent Groups Design – Pretest and Post-test without randomized assignment
For our program, we will implement a quasi-experimental study with a non-equivalent group design. Both the treatment and control group will undergo pre-test and post-test procedures. The scientific notation for our study will be designed as follows:
O1 X O2 O3
O1 O2 O3
Where O1 = the pretest, X = the intervention program (community education in combination with school located vaccination programs), O2 = post-test 6 months after initiation of program, and O3 = post-test 1 year after initiation of program. The treatment group will be Athens-Clarke County elementary schools and the control group will be Jackson county schools. These two groups are obviously not identical, but the income statuses of residents as well as other demographics are similar. Differences between these two communities include racial and ethnic dissimilarities (proportion of minority families) and geographic variations (urban vs. rural) (OASIS, 2011).
Pre-tests will be distributed to parents of elementary school children in Athens-Clarke County and Jackson County 1 month prior to program implementation. Post-test surveys will be distributed 6 months and 1 year after program implementation. Pre-test and post-test surveys will be identical and will assess parents’ knowledge of the seasonal influenza vaccine, parents’ attitude towards the seasonal influenza vaccine, whether or not they have had their children and/or other family members vaccinated against the seasonal flu, and attitudes towards school located vaccination programs.
Online Analytical Statistical Information System (OASIS): Demographic Clusters of Georgia, 2011. Georgia Department of Public Health https://oasis.state.ga.us/gis/demographiccluster/DemoClusters2011.htm
Threats to Internal Validity
Because our program is utilizing a quasi-experimental design, there is a much greater threat to the internal validity of the study versus if we had been able to implement a randomized control trial. This is because we are unable to use random assignment for our treatment and control groups. However, because we are applying pre-test and post-test assignments to both groups, this should help to alleviate potential threats to internal validity.
Selection Bias: This is the most obvious threat to the internal validity of this study as we cannot be sure that our two groups (Athens-Clarke County and Jackson County parents with children in public elementary schools) were comparable before the study was initiated. This will prevent us from determining a cause and effect relationship between the community education in combination with school located vaccination program and an increase in influenza vaccination rates among school children. By implementing the pre and post tests, we reduce this threat slightly.
Testing Bias: The utilization of pre and post tests helps to improve validity of our study, however it also imposes the risk of testing bias. Because parents will be taking a survey prior to the start of the program, they may be primed to think about seasonal influenza vaccination for their children. This could incidentally increase the rate of influenza vaccination among school aged children within our control group.
Attrition Bias: Because the pre-test and post-test will be conducted through voluntary surveys, there is the very likely threat of attrition bias. It is likely that all of the parents that complete the pre-test surveys will not complete one or both of the post-test surveys. There is also the possibility that the children will accidentally lose these surveys or for other reasons not return them to their teachers. This means post-test differences might be due to different levels of dropout.
Table 5: Summary of Measures
| Short-term or Intermediate Outcome Variable | Scale, Questionnaire, Assessment Method | Brief Description of Instrument | Example item (for surveys, scales, or questionnaires) | Reliability and/or Validity Description |
| Decreased levels of misinformation and fear of vaccines. | The Parent Attitudes About Childhood Vaccines Survey (PACV) (Opel, et al. 2011) | This survey was developed in order to better identify “vaccine hesitant parents” so that proper communication and intervention with these providers can be established. While other surveys evaluating attitudes towards immunization exist, this one is specifically designed to target vaccine hesitant parents. | Immunization behavior: “Have you ever delayed having your child get a shot for reasons other than illness or allergy?” Response – Dichotomous: Y/N
Beliefs about Vaccine Safety and Efficacy: “Children get more shots than are good for them.” Response – Likert scale |
Items on the PACV have face and content validity (Opel, et al. 2011). A four-step process was used to determined the style and structure of questions and content included in the survey. Expert panel members evaluated the final content of the survey. Survey participants also determined that the survey was understandable and simple. |
| Increase rates of influenza vaccination among school aged children. | Direct evaluation of influenza vaccination rates among public elementary school children in Athens-Clarke County and Jackson County using the Georgia Immunization Registry (GRITS). | This registry should be utilized by all pediatricians, local public health offices, and other health care providers in the Athens-Clarke and Jackson County areas during the entirety of this program to ensure that comparable data regarding the rates of influenza vaccination among school aged children is comparable between groups. | Vaccine reporting is required by law according to House Bill 1526 stating “any person who administers a vaccine or vaccines licensed for use by the United States Food and Drug Administration to a person.” This should ensure that health professionals in each group are participating. | According to Linkins et al., “immunization registries help ensure high coverage by recording childhood immunizations administered,… calculating immunization coverage and identifying pockets needing immunization services” (Linkins et al., 2006). Because reporting of all FDA approved vaccines is a legal duty of health care professionals, the use of GRITS should be a highly reliable tool. |
| Knowledge and pursuance of appropriate vaccinations for preventable diseases, like influenza. | The Checklist Tool (Gust et al., 2003) | Pediatricians and other healthcare professionals should utilize checklists addressing frequently asked questions posed by parents concerning vaccination so that they are properly prepared with informed yet empathetic responses. There are several different models of checklists including one designed by the Centers for Disease Control and Prevention. | Example checklist FAQs:
– Harmful side effects caused by vaccines. – Bad ingredients in vaccines. – Chances of getting the disease even after vaccination. – |
No data was supplied for the reliability or validity of this measure. |
Opel, D. J., Mangione-Smith, R., Taylor, J. A., Korfiatis, C., Wiese, C., Catz, S., & Martin, D. P. (2011). Development of a survey to identify vaccine-hesitant parents: The Parent Attitudes about Childhood Vaccines survey. Human Vaccines, 7(4), 419–425. http://doi.org/10.4161/hv.7.4.14120
Georgia Immunization Registry, 2016. https://dph.georgia.gov/georgia-immunization-registry-grits
Gust, D. A., Woodruff, R., Kennedy, A., Brown, C., Sheedy, K., & Hibbs, B. (2003). Parental perceptions surrounding risks and benefits of immunization. Semin Pediatr Infect Dis, 14(3), 207-212.
Linkins, R. W., Salmon, D. A., Omer, S. B., Pan, W. K., Stokley, S., & Halsey, N. A. (2006). Support for immunization registries among parents of vaccinated and unvaccinated school-aged children: a case control study. BMC Public Health, 6, 236. http://doi.org.proxy-remote.galib.uga.edu/10.1186/1471-2458-6-236
Process Evaluation and Data Collection Form
** For simplicity, Barrow Elementary School will be used as an example template for all 14 elementary schools in Athens-Clarke county that will be recruited for this intervention.**
Recruitment and Enrollment
A. School Recruitment: Barrow Elementary School Administration will be contacted via letter, phone, and in person. They will receive written letters explaining the program and their participation will be requested. This enrollment includes the educational sessions as well as the school-located clinics.
School Recruitment Letter for Participation in Educational Seminars and School Based Vaccination Clinics
Dear _______,
The University of Georgia College of Public Health, in coordination with the Athens Clarke County Health Department, would like to request your participation in a program study with the goal to increase influenza vaccination rates among children. The intervention program targets children ages 6-11, as well as the parents of these children. The program will include educational material and sessions for parents of elementary school children, providing information on the annual influenza vaccination, hosted over 12 weeks in the fall semester. Following the educational sessions for parents, in-school vaccinations through school based clinics will be administered to participating students with parental consent.
If you are interested in participating in this opportunity, we will be contacting you shortly to discuss more details and address any further questions you may have.
Please contact us at 706-VAX-4FLU or at ProtectAthensKidsFromFlu@uga.edu, for any questions, concerns, or additional information.
Sincerely,
Health Promotion Coordinator
University of Georgia School of Public Health
B. Parent Recruitment: Once a school has been enrolled in the program, school parents will receive letters, provided by us and distributed by the school, explaining the program and their participation will be requested. Letters will be distributed (via paper and emails to parents) within the first month of the start of fall semester.
Parent/Child Recruitment Letter & Form for Educational Seminars and School Based Vaccination Clinics
Dear Barrow Elementary Parent,
The University of Georgia College of Public Health, in coordination with the Athens Clarke County Health Department, would like to request your participation in an exciting new program coming to your child’s school. Barrow Elementary School is proud to announce that we will be participating in a program involving Influenza (Flu) Vaccination for children. This program will include free educational sessions for parents, where important information relevant to influenza vaccination will be provided and commonly asked questions will be addressed. These sessions will also address common misconceptions and explain the importance of influenza vaccines for children from year to year. There will be 12 different informational sessions throughout the fall semester and we ask that each participating parent attend at least one session.
All eligible children, with parental consent will be able receive a free annual influenza vaccine at Barrow County Elementary School. The vaccines will be administered by medical professionals (i.e. doctors, nurses) and will be given during regular school hours in November, December, and January.
Please fill out the attached form and return it to your child’s school, in order to determine your child/children’s eligibility (one form must be completed for every child wishing to receive a vaccine). If you are not interested in participating in this opportunity, please fill out the attached form, detailing your reasons why in the allotted space.
For more information regarding eligibility and answers to frequently asked questions, please visit our website at www.FluVaccines4AthensKids.com.
Please feel free contact us at 706-VAX-4FLU or at ProtectAthensKidsFromFlu@uga.edu, with any questions, concerns, or additional information.
Attached form:
Parent Name: ________________ Parent Phone #:__________
Parent email:________________
Student Name:________________
*Please note that all parents/caregivers with children receiving a vaccine, will be required to attend at least one educational session during the fall semester. However, all parents/caregivers are welcome to attend any educational sessions, regardless of their child’s vaccination status.*
Are you interested in participating in this program? Yes___ No___
If No, please define reason why:
___My child has already been vaccinated for influenza this year
___I do not wish to have my child vaccinated for flu for personal reasons
___I do not wish to have my child vaccinated for flu for religious reasons
___I do not wish to have my child vaccinated for flu for medical reasons
___I will have my child vaccinated elsewhere
___Other:________________________________________________
Student Enrollment Form: To be completed by school upon reception of Initial Parent Contact Form
| Student Name | Student ID # | Parent/Guardian Name | Parent Guardian number | Enrolled (Y/N) | Reason for non-enrollment (if applicable) |
ATTRITION
Each parent will be asked to fill out the following form at the start of the vaccination program at the start of the educational session they choose to attend. They will be asked to fill out another form at the end of the program to prevent loss of follow-up.
Flu Vaccines for Athens Kids Program – Contact Information Form
Parent Name: _____________________
Name(s) of Participating Child(ren):
_____________________ Grade____ DOB_____
_____________________ Grade____ DOB_____
_____________________ Grade____ DOB_____
_____________________ Grade____ DOB_____
_____________________ Grade____ DOB_____
Home Phone:_____________________
Work Phone:_____________________
Cell Phone:_____________________
Email:_____________________
Home Address:_____________________
_____________________
_____________________
Do you plan or anticipate moving to a new address for any reason during this school year? Yes___ No___
If ‘Yes’, provide new address if known:_____________________
_____________________
_____________________
Do you plan or anticipate moving to a new school for any reason during this school year? Yes___ No___
————————————————————————————————————————————————
The following process and form will be used to track parent/guardian attendance at each of the educational sessions during the fall semester and will be filled out by an educational session supervisor upon check-in
| Student Name | Student ID # | Parent/Guardian Name | Parent Guardian email | Date of educational session attended | Parent/Guardian Signature |
*Upon completion of this Flu Vaccine Educational Session, you will receive a confirmation email stating that we have recorded your attendance in our system. Please contact Jon Snow at youknownuthinaboutflu@thewall.net if you do not receive a confirmation email within 48 hours.
The following process and form will be used to track clinic attendance at each of the educational sessions during the fall semester and will be filled out by an accredited medical professional during scheduling and administration of influenza vaccine.
| Eligible Child Name | Eligible Child ID # | Scheduled Vaccination Date/Time | Vaccination Completion/Time | Vaccination Cancellation (Y/N) | Reason for Cancellation (if applicable) | Signature/ID of vaccine administrator |
The following form will be used to collect the surveys distributed at the beginning of the school year (August screening survey), after the educational sessions and school located clinics (January survey), and at the beginning of the following school year (next August follow up survey) measuring attitudes towards vaccinations, including general knowledge, perceived barriers, and perceived benefits. The survey results will be recorded and entered into a data spreadsheet and translated using a data dictionary.
| Parent Name | Child(ren) ID Numbers | August 2017 Survey Submitted (Y/N) | January 2018 Survey Submitted (Y/N) | August 2018 Survey Submitted (Y/N) |
PROGRAM FIDELITY
Program Fidelity Checklist Form
Educational Session Components
(100-70%), (40-69%), or (<40%)
____ 1. Were proper curriculum resources available to conduct meaningful educational sessions?
____2. Were “Before” surveys completed and submitted by parents?
____3. Were “After” surveys completed and submitted by parents?
____4. Were questions raised by parents addressed in an appropriate and effective manner?
- Were there any barriers or difficulties that prevented delivery of effective educational information at any of the educational sessions? ____yes ____no
If ‘Yes’, please explain: ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Vaccination Sessions at School-Based Clinics
(100-70%), (40-69%), or (<40%)
____6. Were all eligible children provided with an influenza vaccination, free of charge?
____7. Were the vaccinations administered in a timely and effective manner as to detract from regularly scheduled class time as little as possible?
____8. What was the level of student vaccination at the vaccination sessions, school-wide?
**As this is a one time vaccination, no follow-up will be provided to parents outside of what may be mentioned in regular school newsletters provided by the school.**
SOURCES:
“2016 Recommended Immunizations for Children from Birth Through 6 Years Old,” CDC
Rand CM, Shone LP, Albertin C, et al. National health care visit patterns of adolescents: implications for delivery of new adolescent vaccines. Arch Pediatr Adolesc Med 161:252-259. 2007.
“Flu Vaccination Coverage* by Race/Ethnicity, Children 6 months–17 years, United States,† 2014–15 Season.” CDC. 2016. http://www.cdc.gov/flu/fluvaxview/coverage-1415estimates.htm#data
Longini, I. M., Jr., & Halloran, M. E. (2005). Strategy for distribution of influenza vaccine to high-risk groups and children. Am J Epidemiol, 161(4), 303-306. doi:10.1093/aje/kwi053
Online Analytical Statistical Information System (OASIS): Demographic Clusters of Georgia, 2011. Georgia Department of Public Health https://oasis.state.ga.us/gis/demographiccluster/DemoClusters2011.htm
Opel, D. J., Mangione-Smith, R., Taylor, J. A., Korfiatis, C., Wiese, C., Catz, S., & Martin, D. P. (2011). Development of a survey to identify vaccine-hesitant parents: The Parent Attitudes about Childhood Vaccines survey. Human Vaccines, 7(4), 419–425. http://doi.org/10.4161/hv.7.4.14120
Georgia Immunization Registry, 2016. https://dph.georgia.gov/georgia-immunization-registry-grits
Gust, D. A., Woodruff, R., Kennedy, A., Brown, C., Sheedy, K., & Hibbs, B. (2003). Parental perceptions surrounding risks and benefits of immunization. Semin Pediatr Infect Dis, 14(3), 207-212.
Willis, E., Sabnis, S., Hamilton, C., Xiong, F., Coleman, K., Dellinger, M., … Simpson, P. (2016). Improving Immunization Rates Through Community-Based Participatory Research: Community Health Improvement for Milwaukee’s Children Program. Progress in Community Health Partnerships : Research, Education, and Action, 10(1), 19–30. http://doi.org.proxy-remote.galib.uga.edu/10.1353/cpr.2016.0009
Aragones, A., Bruno, D. M., Ehrenberg, M., Tonda-Salcedo, J., & Gany, F. M. (2015). Parental education and text messaging reminders as effective community based tools to increase HPV vaccination rates among Mexican American children. Preventive Medicine Reports, 2, 554–558. http://doi.org.proxy-remote.galib.uga.edu/10.1016/j.pmedr.2015.06.015
Yoo, B.-K., Humiston, S. G., Szilagyi, P. G., Schaffer, S. J., Long, C., & Kolasa, M. (2015). Cost effectiveness analysis of Year 2 of an elementary school-located influenza vaccination program–Results from a randomized controlled trial. BMC Health Services Research, 15, 511. http://doi.org.proxy-remote.galib.uga.edu/10.1186/s12913-015-1169-5
Linkins, R. W., Salmon, D. A., Omer, S. B., Pan, W. K., Stokley, S., & Halsey, N. A. (2006). Support for immunization registries among parents of vaccinated and unvaccinated school-aged children: a case control study. BMC Public Health, 6, 236. http://doi.org.proxy-remote.galib.uga.edu/10.1186/1471-2458-6-236