
Part I. Community Guide Update and Rationale for Intervention
Table 1: Summary of Recent Interventions:
| Author & Year | Intervention Setting, Description, and Comparison Group(s) | Study Population Description and Sample Size | Effect Measure (Variables) | Results including Test Statistics and Significance | Follow-up Time |
| Rehn et al., 2016 | The Swedish vaccination program offers free HPV vaccinations to girls, specifically targeting those that were born from 1993 to 1998. An etiological study was done with data being done by county. | All 21 county health care offices replied to the surveys. While only four schools offered HPV vaccinations to the catch-up group, all 21 offered vaccination to the catch-up group through primary health care settings. | Vaccine Uptake | The counties in which vaccinations were offered in all schools and in just some schools had higher vaccine uptake than counties (all schools adjusted IRR: 1.3, 95% CI: 1.1–1.5, some schools adjusted IRR: 1.2, 95% CI: 1.1–1.3). | 3 years |
| Saad et al., 2006 | They analyzed rates of nonmedical exemptions versus pertussis incidence data for those 18 and younger | States with no non-medical exemptions versus states with religious exemptions and personal-belief exemptions. Also states with easier processes of receiving nonmedical exemptions were compared to those with medium difficulty or difficulty processes for receiving a nonmedical exemption | Vaccine Uptake, Pertussis Incidence | States with an easier granting of exemptions (incidence rate ratio = 1.53; 95% confidence interval, 1.10-2.14) and states with personal belief exemptions (incidence rate ratio = 1.48; 95% confidence interval, 1.03-2.13) were associated with increased pertussis incidence. | 2 years |
| Zimmerman et al., 2014 | 20 pediatric and family medicine practices were contacted to be involved in an intervention in which the 4 Pillars Immunization Toolkit (a practice improvement toolkit, early delivery of donated vaccine for disadvantaged children, staff education, and feedback on progress) was put into place. They measured influenza vaccine uptake and the maintenance of it in children aged 6 months to 18 years. | 20 pediatric and family medicine practices were involved in this study. these were randomized to receive the intervention in either year 1 or year 2. | Vaccine uptake of influenza, vaccine maintenance of influenza | Vaccine uptake increased by 8% (P < .01) during intervention and was sustained (+0.4 PP; P > .05) during maintenance. | 10 years |
Community Guide Update and Rationale for Intervention:
Vaccination requirements for child care, school, and college attendance is currently recommended by the Community Preventive Services Task Force as of 2016 due to evidence suggesting it increases vaccine coverage, as well as benefiting ethnic and racial minorities. This review is based on 32 different studies done from 1980 to 2015, only one of which focused on colleges; however, it is probable that we will see increased vaccine uptake in colleges as well. Despite this, there are three aspects of vaccination requirements that may influence vaccination rates: 1) geographic clustering of under-immunization, 2) inconsistent enforcement of requirements, and 3) the relative ease of obtaining nonmedical exemptions. It is recommended that we increase the difficulty of receiving a medical exemption pass, as well as making enforcement and monitoring more clear and consistent.
The study published by Rehn et al. focuses on increasing HPV vaccinations in Swedish girls by making offering these vaccinations to a catch-up group. This study was done in all counties in Sweden, focusing on girls born between 1993 and 1998 with a three-year follow-up. All primary health-care centers provided these vaccinations, but only four schools did so. The schools that did showed an increase in HPV vaccination compared to counties in which no schools offered these. This is indicative of school’s important role in children’s vaccinations and how children receive them. Based on this, we recommend an increase in school’s participation in childhood vaccinations; however, we cannot directly apply this to vaccination requirements in schools.
The article published by Saad et al. analyzed rates of nonmedical exemptions versus pertussis incidence data for children 18 and younger. States with no nonmedical exemptions were compared to states with religious nonmedical exemptions and states with both personal belief and religious nonmedical exemptions. The process of getting a nonmedical exemption was also compared, ones that were rated as difficult were compared to those rated medium and easy difficulty. States with an easy process of getting a nonmedical exemption or personal belief nonmedical exemptions were associated with a higher incidence of pertussis. Though this study focuses only on pertussis incidence, it is reasonable to assume there might be a similar incidence in other vaccine-prevented diseases. This study recommends banning nonmedical exemptions, if not making it more difficult to receive them.
The study by Zimmerman et al. studies how the 4 Pillars Immunization Toolkit (a practice improvement toolkit, early delivery of donated vaccine for disadvantaged children, staff education, and feedback on progress) affects vaccine uptake. 20 pediatric and family medicine centers were tasked to implement the toolkit. Vaccine uptake and maintenance were measured in children aged 6 months to 18 years. During this intervention, vaccine uptake increased by 8% and maintained. This study recommends a more involved approach to children’s vaccinations, especially those that are recommended when it comes to healthcare providers.
Part II. Theoretical Framework/Model
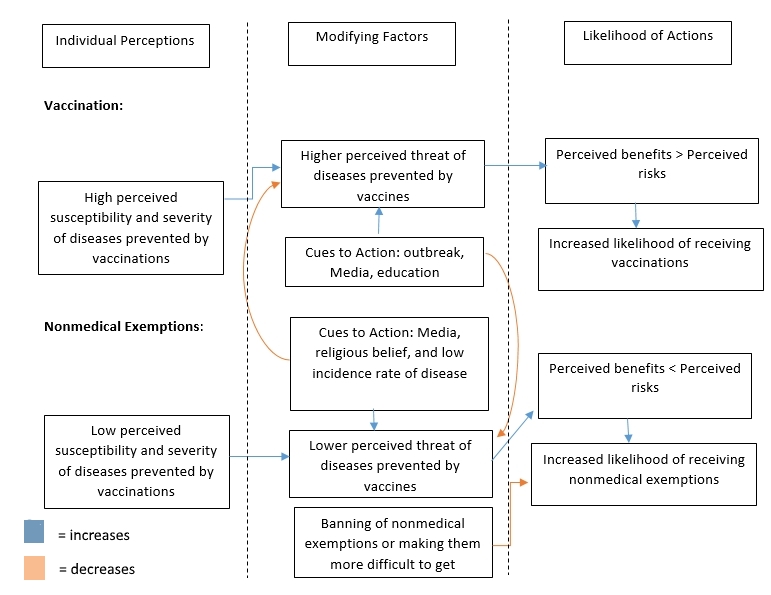
We will be exploring the effects of nonmedical exemptions on childhood vaccination and sickness, so this will be explored using the Health Belief Model. The Health Belief Model attempts to explain and predict health behaviors. It focuses on the attitudes and beliefs of individuals. We believe this is the best fit for nonmedical exemptions and vaccinations, as many vaccinations (such as Hepatitis A and Measles, Mumps, Rubella) are free with insurance with no copayments as required by law. Many scientists support vaccinations and their benefit to society. However, the United States still has an issue with vaccine uptake and, recently, nonmedical exemptions leading to outbreaks of diseases prevented by vaccinations. There are five main constructs, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, and cues to action.
Constructs:
Perceived susceptibility, how much one believes they are susceptible to a disease, can affect how likely one is to get a vaccine. For example, parents may not get their children the HPV vaccine, due to the belief that their child will not have sex, or at least not having sex at the moment. more on this
Perceived severity, how severe a person believes a condition is, may also play a role in vaccination. A parent who has never seen pertussis in their lifetime may be under the impression that it is not that bad, after all it doesn’t get the news coverage or shows that smallpox does. Similarly, someone who is unfamiliar with diseases may believe the black plague is very severe and a death sentence, when most times it can be cured with antibiotics.
The amount of nonmedical exemptions also depends on the difficulty of getting a nonmedical exemption, and how often a nonmedical exemption has to be renewed, which can be applied to the construct of perceived barriers to getting a nonmedical examination. more on this
It will also be affected by the general attitude toward vaccination. Nonmedical exemptions tend to be clustered in groups, showing that it may be partially due to that area’s general outlook on vaccinations. This may be caused by the belief that the vaccination causes harm, or does not work. People who don’t vaccinate may also think it is better for their immune system to fight off diseases. Both of these examples can be seen as perceived benefits to receiving a nonmedical examination. Sickness due to not being vaccinated can depend on how many people are not vaccinated in the area.
Diagram of Conceptual Model:
Part III. Logic Model, Causal and Intervention Hypotheses, and Intervention Strategies
Target Population:
Our intervention will target areas in which there is a high amount of nonmedical exemptions in California. These areas face a greater risk of disease due to their high amount of unvaccinated children, which tend to be white, middle-class Americans. We will be targeting children aged 0 to 10 who live in these areas, focusing on white, middle-class Americans, because most vaccinations for severe preventable diseases such as measles are scheduled before kindergarten in the United States.
Intervention Setting:
The weekly talks and discussions given by trained volunteers will be done in various key locations in the community, specifically churches, schools, rotary clubs, etc. These places will be easily accessible and comfortable places for the parents while also still acceptable places to learn. Talks between the parent and a doctor or public health professional will take place in the office of the doctor or public health professional. These offices will help parents feel more comfortable in a one-on-one discussion with a trained professional.
Table 2: Intervention Methods and Strategies:
| Intervention Method | Alignment with Theory | Intervention Strategy |
| Increased perceived barriers to getting a nonmedical exemption | By increasing the perceived barriers to getting a nonmedical exemption, those who do not believe in vaccinations will see a nonmedical exemption as difficult to get or not worth it, especially if this belief is not strong. A parent who has a slight belief in a nonmedical exemption may be more likely to seek it if it is light paperwork done only once per child, but will most likely see it as not worth it if paperwork is heavy, involves meeting people, and/or has to be done yearly per child.
Rather than increasing the difficulty of getting a nonmedical exemption, by simply banning nonmedical exemptions, the perceived barriers to getting a nonmedical exemption would increase for a parent. A parent who wants to avoid getting vaccinations for their children would have to go to a private school or homeschool their children in order to do so, meaning the belief in forgoing vaccinations would have to be very strong in order for a |
|
| Increase preceived benefits of vaccinations | Parents who are unaware of diseases prevented by vaccinations are more likely to seek a nonmedical exemption, especially for diseases these parents may have never dealt with personally. By having a doctor speak personally to a parent or a public health professional, showing them videos of patients with the disease, infection rate, mortality rate, and symptoms of these diseases, a parent may be convinced that the vaccination would be worth the risks the parent believes in. This would be even more likely if this was required to happen before a child is approved for a nonmedical exemption, which would be a perceived barrier. | Have doctors speak to patients about diseases prevented by vaccinations by reaching out to doctors in the community, or with news and interviews from public health professionals about these diseases, outbreaks of these diseases, and the risks of these diseases |
| Increase perceived severity and susceptibility of diseases prevented by vaccinations | We will seek to increase perceived benefits by a parent by having talks/lectures in the community via schools, churches, rotary clubs, etc. By doing this, we will hopefully host these lectures in places where people normally go anyways and are comfortable in rather than a doctor or public health professional that they may see as callous or feel uncomfortable with. To further that agenda, we will be seeking volunteers who we will train to give these lectures about vaccinations. In theory, these talks will increase the perceived benefits of vaccinations by parents who are thinking of getting a nonmedical exemption, perhaps even outweighing the perceived risks of vaccination. | volunteer lectures in the community |
Table 3: Program Logic Model:
| Inputs/Resources | Activities | Outputs | Short-term Outcomes | Intermediate Outcomes | Long-term Outcomes |
| funding from government, input and time from public health professionals in community, input from government officials, funding from public health organizations, time and cooperation from doctors, schools, community, and clubs. Time from volunteers | change policy so that nonmedical exemptions are not allowed or are more difficult to get (such as increase paperwork, process of getting exemption, and/or increase how often a medical exemption needs to be renewed). talks with doctors and public health professionals about vaccines with patients, lectures in schools, community, clubs, etc. | 20 lectures given to the community over the course of the year, all representatives of California’s house and senate contacted via email or more, 50 doctors and public health professionals contacted, increase in positive feelings of vaccinations | Evidence of increase in perceived barriers to getting a nonmedical exemption
Evidence in increase in perceived benefits of getting a vaccination evidence in increase of perceived severity and susceptability of diseases easily prevented by vaccinations |
Decrease nonmedical exemptions
increase in vaccinations that are required anyways increase in vaccinations that are not required by the school |
Decrease amount of outbreaks of preventable diseases from vaccination, decrease prevalence of preventable diseases from vaccination, increase quality of life for children who are immunocompromised and live in communties with clusters of nonmedical exemptions |
Intervention Hypothesis:
By changing policy so that nonmedical exemptions are either more difficult to receive or outright banning them will increase the perceived barriers to getting a nonmedical exemption. However, increasing lectures with volunteers will increase perceived benefits of getting vaccinated and increasing personal talks with doctors and public health professionals will increase the perceived severity and susceptibility of diseases prevented by vaccinations.
Causal Hypothesis:
Changing policy so that nonmedical exemptions are not allowed will decrease nonmedical exemptions and thus increase vaccinations by increasing perceived barriers to getting a nonmedical exemption. However, this will not increase knowledge of vaccinations or vaccinations that are not required by schools.
If we changed policy so that nonmedical exemptions are more difficult to get via increasing paperwork, increasing the process, and/or increasing how often a nonmedical exemption has to be renewed will increase vaccinations by decreasing nonmedical exemptions. We expect that increasing the difficulty of getting a nonmedical exemption (through such methods as increasing paperwork, increasing the process, or increasing the frequency it has to be renewed) will decrease nonmedical exemptions, especially for parents who are not as strong in their belief in the risks of vaccinations as others. However, we expect banning nonmedical exemptions from public schools will decrease nonmedical exemptions more so as it will take care of any parent who wishes to not get their child vaccinated, except those who are so strong in belief that they will place their child in a private school (who may take their child unvaccinated) or even homeschooling them. This method would increase vaccine uptake, but may actually increase situations in which there are many children in one localized area who are not vaccinated, as these strongly-willed parents will send their unvaccinated children to one place. This also does not increase the knowledge of vaccinations in these parents.This is not expected to increase knowledge of vaccinations or vaccinations that are not required by the schools, however.
Increasing lectures given by trained volunteers around the community is expected to lead to an increase in all vaccinations, including those not required by schools, and a decrease in nonmedical exemptions.
Increased personal talks from doctors and public health professionals will lead to an increase in vaccinations, including those that are not required in schools, and a decrease in nonmedical exemptions. This seems like a good method to increasing vaccinations, which include vaccines that are not typically required by schools, such as the HPV vaccination.
Smart Objectives:
Goal 1: Increase in perceived severity and susceptibility of diseases prevented by vaccinations
Objective 1: After intervention implementation, 70% of parents will pass a test on different diseases prevented by vaccinations with a score of at least 75%
Objective 2: At 4-month follow-up, parents will show an average of 20% increase in a survey on perceived risk of diseases prevented by vaccinations
Goal 2: Increase in perceived benefits of vaccinating a child
Objective 1: After intervention implementation, parents respond more positively in a survey to vaccinations by 25% on average
Objective 2: at 4-month follow-up, the percentage of parents who respond more positively in a survey to vaccination by 25% on average will not have decreased by more than 5% than reported after intervention implementation
Goal 3: Increase in perceived barriers to nonmedical exemptions
Objective 1: During the course of our intervention, 50 senators or house of representatives for the state of California will be contacted in order to push for increasing the difficulty of nonmedical exemptions or outright banning them.
Part IV. Evaluation Design and Measures
Table 4: Stakeholder Roles:
| Stakeholder | Role in Intervention | Evaluation Questions from Stakeholder | Effect on Stakeholder of a Successful Program | Effect on Stakeholder of an Unsuccessful Program |
| Public health professionals /teachers/ doctors/ volunteers to lecture | Will help with intervention by either giving personal talks (in the case of doctors and public health professionals) or lectures (in the case of trained volunteers or teachers) | How can I be involved? What is my time and money input for this? How do I reach out to parents? | Increase in participation and knowledge of the program. More willing to recommend program | May not participate in the future or will lose confidence in intervention |
| State senators and representatives in California’s government | Can decide public policy that has to do with our intervention | How do my constituents feel about these issues? How does my support help this intervention? | Increase in positive thoughts toward vaccination, more willing to suggest policy that is positive toward vaccinations | No change in thoughts towad vaccination. Will not suggest policy that is positive toward vaccinations. |
| Parents (especially those seeking nonmedical exemptions) | Those we seek to reach out to participate in our program | How will my child be affected by vaccinations? What are the benefits of vaccination? | Increase of positive thoughts toward vaccination, increase in child vaccinations (including those not required) and decrease in nonmedical exemptions | No change in the amount of nonmedical exemptions or amount of unrequired vaccination. Opinions toward vaccination remain unchanged |
| Schools/ child care/ churches/ community | will be affected by results/ may help out in program | How will parents react to my support? How can I support this program? What is my time and monetary input in this program? How will the children be affected by this? | Increase in willingness to talk to parents about vaccination in a positive light, increase in positive conversation about vaccinations in general, more opportunities to give lectures and such | Time and money wasted along with decrease in willingness to support the program |
Evaluation Design: Group Randomized Control Trial
R O1 X O2 O3 (Intervention group A)
R 01 X O2 O3 (Intervention group B)
R 01 X O2 O3 (Intervention group C)
R O1 O2 O3 (Control group)
[O1 = pre-test and pre-survey, O2 = post-test after intervention, O3 = post-test and post-survey at 16 weeks]
Intervention Group A: Lecture from trained volunteers about vaccines and their elected senator and representative contacted about nonmedical exemptions
Intervention Group B:Personal talk with health care provider (such as their doctor) and their elected senator and representative contacted about nonmedical exemptions
Intervention Group C: Both lecture from a trained volunteer about vaccines and a personal talk with their health care provider
Control Group: Will continue with normal education on vaccines
Threats to Internal Validity:
We will randomize groups by county so that parents of students will be less likely to cross contaminate. These groups should face similar threats to internal validity, but we will conduct a pre-test analysis in order to test how similar these groups are before our intervention started.
Information Bias: Other Sources of Information:
Besides our intervention, there are many sources of information about vaccines that a parent can go to. These sources may highlight the benefits of vaccinating or focus on the negative aspects or theories on vaccination. A parent may be actively seeking this information by going on the internet or t0 the library, but equally likely is that a parent may be simply watching the news or browsing a news website, as vaccination and diseases are both hot topics for journalists. However, it will be hard to keep parents from talking to their health care provider on their own agenda (not managed by us) or picking up brochures or information from the internet, so we must address this by asking in the surveys to account for this.
Timing Bias: Outbreak of Disease Prevented by Vaccination:
Over the course of our intervention and afterward, we must be aware of outbreaks of vaccine-prevented diseases that occur. We cannot control these outbreaks, but we must consider it if this does occur, as it will likely cause an increase in vaccinations that we will falsely contribute to our intervention.
Mortality/Attrition:
As in all interventions and studies, there is a chance that participants will die or simply lose touch with us. We hope by contacting parents initially through their children’s school, we will be less likely to lose touch with these parents. Additionally, the settings of these interventions should contribute to less attrition as their contact information should be available. We will be looking at our pre-test data to make sure there is not a difference in drop-out rate between our interventions.
Testing:
By using a pre-test and post-test, we run the risk of setting up parents to look for the information we tested them on in their lectures and/or personal talks. This may cause post-tests to have better results even if the intervention was not effective. By using a pre-survey and post-survey, we may also cause parents to think more critically about their answers on their pre-survey before their post-survey, perhaps changing their answers simple due to being given this survey instead of our intervention.
Table 5: Summary of Measures:
| Short-term or Intermediate Outcome Variable | Scale, Questionnaire, Assessment Method | Brief Description of Instrument | Example item (for surveys, scales, or questionnaires) | Reliability and/or Validity Description |
| Increased perceived benefits of vaccines, increased perceived barriers of nonmedical exemptions | The Parent Attitudes about Childhood Vaccines survey (Opel et al., 2011) | This survey with 18 questions was designed to measure vaccine hesitancy using four domains: n four content domains: immunization behavior; beliefs about vaccine safety and efficacy; attitudes about vaccine mandates and exemptions; and trust | Immunization Behavior: If you had another infant today, would you want him/her to get all the recommended shots? Y/N/DK
Belief about Vaccine Safety and Efficacy:It is better for my child to develop immunity by getting sick than to get a shot. SA/A/NS/D/SD Attitudes about Vaccine Mandates and Exemptions: The only reason I have my child get shots is so they can enter daycare or school. Y/N/DK Trust: I trust the information I receive about shots. SA/A/NS/D/SD |
The mean PACV score was 23.8 at first and then 21.9 after 8 weeks (ρ = 0.844 [95% CI, 0.806-0.882]). Both the baseline and 8-week PACV subdomain scores were highly concordant at 0.791 (95% CI, 0.742-0.841), 0.826 (0.784-0.868), and 0.625 (0.545-0.705) |
| Increased perceived severity and susceptibility to diseases prevented by vaccines, increased vaccinations | Survey from the study “Immunization Knowledge and Practice among Malaysian Parents”, modified to better fit our target participants. (Awadh et al., 2014) | A questionnaire with 20 questions, 10 on knowledge and 10 on practice. Parents with children aged 2 to 5 and lived in Pahang were included in this survey. | Knowledge: find pertussis incidence
Practice: Is your child up-to-date with all their vaccinations? Y/N/DK |
For knowledge and practice, internal consistency was found to be good (Cronbach’s alpha = 0.757 and 0.743 respectively); the test-retest reliability value was 0.740 (p = 0.014). |
Part V. Process Evaluation and Data Collection Forms
- Provide the following data collection forms for monitoring the program process. More than one form may be submitted for a given category, but all forms must be clearly labeled. (18 points)
- Recruitment and enrollment – how will you track who you invite to participate in your intervention and who actually takes part?
School recruitment:
Vaccine Uptake Program in Children
School Recruitment Letter
Dear _______________,
The University of Georgia’s School of Public Health would like to invite you to be part of our vaccine uptake program, which aims to increase childhood vaccinations in ages 0 to 10. This program includes lectures and small group sessions conducted over a period of two weeks. If you are interested in this program and would like to learn more, please join us on June 4, 2016 at 7 pm at the University of Georgia’s Health Sciences Campus at Russel Hall room 255.
You can also contact us by calling 1800-555-VACC or at Vaccinechildren@uga.edu.
School Enrollment Form:
| School Name | School Contact Number | Number of Children |
|---|---|---|
Schools that sign up for this program will then send out this letter with the children to their parents:
Dear Parent/Guardian,
In partnership with (school name), we are hosting a vaccine educational program, which we would like to invite you and your child to partake in.
As part of the program, you will be participating in (lecture and/or talk with doctor depending on which group they’re in). This will be done at school at 5 pm for two Tuesdays in a row. You and your child will receive assessment tests before your program, afterwards, and two months after this program is complete.
Please fill out the form below if you are interested in participation.
For more info, contact vaccinechildren@uga.edu.
Student name: _____________________________________________________
DOB: _____________
Parent/Legal guardian name: ______________________________________________________________
Doctor Participation form for personal talks with family doctors:
Dear _______________,
The University of Georgia’s School of Public Health would like to invite you to be part of our vaccine uptake program, which aims to increase childhood vaccinations in ages 0 to 10. We would like to invite you to speak with participants of this program about vaccines and the diseases they prevent. If you are interested in this program and would like to learn more, please join us on May 13, 2016 at 7 pm at the University of Georgia’s Health Sciences Campus at Russel Hall room 255.
You can also contact us by calling 1800-555-VACC or at Vaccinechildren@uga.edu.
We will also contact the doctors via phone in order to get the most doctors on board for counties that will be given personal talks with doctors.
Volunteer Participation Form:
Dear _______________,
The University of Georgia’s School of Public Health would like to invite you to be part of our vaccine uptake program, which aims to increase childhood vaccinations in ages 0 to 10. We would like to invite you to speak with participants of this program about vaccines and the diseases they prevent. If you are interested in this program and would like to learn more, please join us on May 5, 2016 at 7 pm at the University of Georgia’s Health Sciences Campus at Russel Hall room 255.
You can also contact us by calling 1800-555-VACC or at Vaccinechildren@uga.edu.
School enrollment form
| School Name | Name of Child | Name of Parent |
|---|---|---|
Each Parent will be asked to sign in for the two lectures.
Lecturers will be given this to fill out after each lecture:
| Lecture Components | Agree | Neutral | Disagree |
|---|---|---|---|
| Was the curriculum available? | |||
| Scheduled lectures were completed | |||
| Group discussions were completed | |||
| There were no technical difficulties | |||
| Group participation was high | |||
Schools that are having personal talks with their doctors will have the doctors fill out this form after the end of our intervention:
| Question | Answer |
|---|---|
| In general, how well did parents respond to your talks from a scale of 1 (being very bad) to 5 (very good)? | |
| Were parents given enough time for questions? | |
| To your best knowledge, on a scale of 1 to 5, how thorough were you in explaining vaccines and the diseases prevented by them? | |
| On a scale of 1 to 5, how well did you feel parents understood what you were saying. |
And will fill out this form to see how many parents were involved in this implementation:
| Doctor's name | Doctor's County | Name of Participant | Date Enrolled |
|---|---|---|---|
All schools except the control group will have the state senators and representatives fill out this form after the intervention:
| Question | Answer |
|---|---|
| From the information given to you over the course of this intervention, do you feel you were given enough information to make an informed decision on policy regarding nonmedical exemptions | Y/N/DK |
| Based on this information, would you recommend banning nonmedical exemptions? | Y/N/DK |
| Based on the information given, would you recommend making the process of getting a nonmedical exemption more difficult? | Y/N/DK |
Citations:
Awadh A, Hassali M, Al-Lela O, Bux S, Elkalmi RM, Hadi H. Immunization knowledge and practice among Malaysian parents: a questionnaire development and pilot-testing. BMC Public Health. 2014;14(1):1107. doi:10.1186/1471-2458-14-1107.
Omer SB, Pan WKY, Halsey NA, et al. Nonmedical Exemptions to School Immunization Requirements.Jama. 2006;296(14):1757. doi:10.1001/jama.296.14.1757.
Opel DJ, Taylor JA, Zhou C, Catz S, Myaing M, Mangione-Smith R. The Relationship Between Parent Attitudes About Childhood Vaccines Survey Scores and Future Child Immunization Status. JAMA Pediatrics JAMA Pediatr. 2013;167(11):1065. doi:10.1001/jamapediatrics.2013.2483.
Opel DJ, Taylor JA, Zhou C, Catz S, Myaing M, Mangione-Smith R. The Relationship Between Parent Attitudes About Childhood Vaccines Survey Scores and Future Child Immunization Status. JAMA Pediatrics JAMA Pediatr. 2013;167(11):1065. doi:10.1001/jamapediatrics.2013.2483.
Rehn M, Uhnoo I, Kühlmann-Berenzon S, Wallensten A, Sparén P, Netterlid E. Highest Vaccine Uptake after School-Based Delivery – A County-Level Evaluation of the Implementation Strategies for HPV Catch-Up Vaccination in Sweden. PLOS ONE PLoS ONE. 2016;11(3). doi:10.1371/journal.pone.0149857.